
The 17,000 ‘hydroxychloroquine deaths’ that never happened

We published our first article asking whether the cheap generic anti-malaria drug, hydroxychloroquine (HCQ), was an effective treatment for covid and whether it was already saving lives on April 16, 2020. Mainstream journalists had been displaying a strange reluctance to ask serious questions about it. Over the next months the establishment health authorities and ‘covid’ scientists did their best to trash the drug, with great success, and we now know why – it would have interfered with their mRNA vaccine development and marketing that was set to make billions for Big Pharma and their government acolytes. It was a story we reported on TCW from the start – how Donald Trump’s advocacy of the drugs was all that was needed for the MSM to go into gleeful overdrive rubbishing it. However the President’s unexpected retweet of our May 2020 investigative article on HCQ’s potential benefits for tackling covid did draw attention to it. The retraction of the Lancet and New England Journal of Medicine’s articles on the Oxford RECOVERY trials which put paid to the treatment, and to the truth about the flawed RECOVERY claims, Edmund Fordham reported in TCW in June 2020, going on to report on the trials’ further iniquitous procedures and claims here and here.
It was therefore heartening to see this further vindication in the Brownstone Institute last week, coming nearly four years after our original exposé.
***
EARLY this year, Americans learned about the publication of an article from Elsevier’s Journal of Biomedicine and Pharmacotherapy overseen by Dr Danyelle Townsend, a professor at the University of South Carolina College of Pharmacy’s Department of Drug Discovery and Biomedical Sciences. As Editor-in-Chief, Dr Townsend reviewed, approved and published the article titled: ‘Deaths induced by compassionate use of hydroxychloroquine [HCQ] during the first COVID-19 wave: An estimate‘.
The article was a hypothesised estimate of people that might have died, but now even that estimate has been retracted. The reason given for the retraction was that the Belgian dataset that was one of the bases for the piece was found to be ‘unreliable‘; in reality it was fraudulent. The article also repeatedly referenced the New England Journal of Medicine’s 2020 RECOVERY trial. The RECOVERY trial is well known to be a deeply flawed study which, in addition to implementing late treatment in severely ill Covid patients, used extremely high doses of HCQ.
The authors of the retracted publication were all French or Canadian, with the primary author a pharmacist by the name of Alexiane Pradelle. According to a rudimentary internet search, Dr Pradelle had never published before. Subsequently, listed authors were degreed as physicians, pharmacists, and/or professors of their respective disciplines. The main, corresponding author, Jean-Christophe Lega, runs the Evaluation and Modeling of Therapeutic Effects team at the University of Lyon.
Hydroxychloroquine’s fabled safety history contrasts data
In addition to being a hypothesised estimate, the article attacked the legendary safety of HCQ, contradicting centuries of the safety of quinolines as a class.
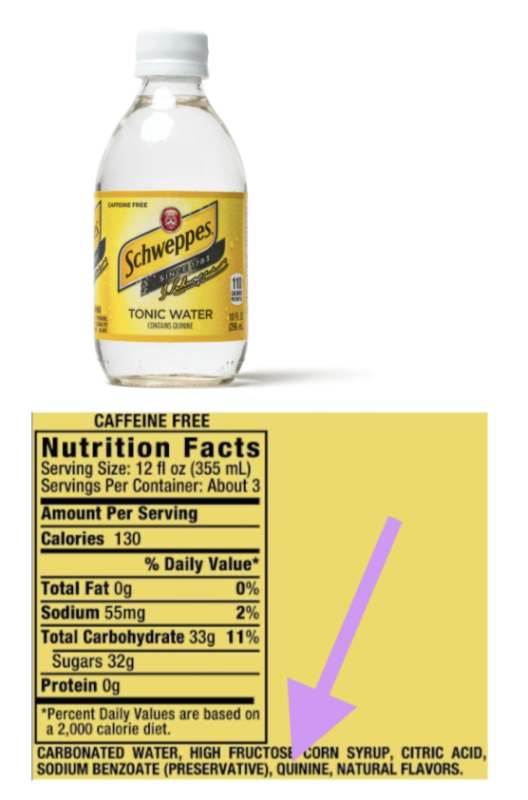
HCQ, chloroquine and quinine are structurally and pharmaceutically/mechanistically related, sharing the same quinoline structural group. The original iteration of quinine was a very fortunate discovery that dates back to the 1600s (at least) as a medicinal tipple used by Jesuit missionaries in South America. It is naturally found in the bark of the Cinchona tree (also called a ‘Quina-Quina’ tree).
Quinine is still available both as a prescription drug, for similar indications as HCQ including malaria . . . and as a Covid-19 treatment.
Quinine is so safe that it may be unique in that the FDA simultaneously permits its use without a prescription, as an ingredient in tonic waters.
HCQ is similarly safe when used appropriately and under medical supervision.
The Centers for Disease Control (CDC) describes HCQ as ‘a relatively well tolerated medicine‘ and that ‘HCQ can be prescribed to adults and children of all ages. It can also be safely taken by pregnant women and nursing mothers‘, referring to its long-term use in chronic diseases.
Basic logic dictates that, if a drug is safe for long-term use, it would also be safe for short-term use, including (and especially) in Covid-19 early treatment/pre-exposure prophylaxis type indications.
These are pharmacology fundamentals that ought to be known by any pharmacist or physician – let alone by a professor serving as a journal Editor-in-Chief at a taxpayer-funded state College of Pharmacy.
Did not even one person on her editorial board of more than 50 ‘peer-reviewers’ and staff ponder the celebrated and storied history of HCQ (and its predecessors) and how incongruent this study’s findings were before choosing to publish data denigrating HCQ safety?
The correct answer to that might actually be: No.
The publishing editorial board all seem to be laboratory bench (non-clinical) research scientists, per their biographies. Although the board does promote itself as meeting DEI requirements of being ‘gender diverse‘, a more important question might be is if they have the appropriate credentials and experience to review and opine on clinically complex drug safety/epidemiology subject matters in the first place.
Is just anyone now allowed to opine on specialty clinical pharmacology drug safety matters?
In certain journals/news publications, the answer to that question seems to be: Yes.
Those ‘17,000 Deaths’ never occurred
Another point of confusion surrounded the interpretation and promotion of this little-known publication by the lay press.
To be exact: there were never ‘17,000 deaths’; it was always a hypothetical extrapolation of people that could have died, based on ‘unreliable’ (actually, fraudulent) databases on top of the previously mentioned, problematic late-stage RECOVERY-trial-type dosing and timing.
Still, Josh Cohen, a Forbes.com PhD senior healthcare columnist, used this publication to headline an absurdly biased op-ed against HCQ, stating that Trump’s HCQ proposal was ‘Linked To 17,000 Deaths‘. The Tufts, Harvard, and the University of Pennsylvania- trained ‘healthcare analyst‘ misrepresented or appeared not to understand the now-retracted study methodology or projections.
It went downhill from there. Mere hours following the publication, very similar, now objectively inaccurate, highly politicised, and seemingly coordinated attacks on HCQ and Trump were published by: The Hill, Politico, Frontline News, Scripps News, the Guardian, KFF Health News, News Nation, Newsweek, AOL.com, Yahoo News, and Daily Kos, in addition to a multitude of prominent regional, international and US federal news outlets, many falsely estimating that 17,000 deaths had already taken place and that the (imaginary) victims’ blood was already on Donald Trump’s hands.
As of September 15, 2024, the above and other articles still show up very prominently (on the first page) of a Google search for ‘hydroxychloroquine deaths’ . . . which never happened.
Here are some screenshots of headlines referencing non-existent deaths based on a now-retracted study:




Journal editors were immediately warned about questionable findings
Almost immediately following the publication on January 2, 2024, the article’s critical flaws including basic miscalculations among many other deficiencies were brought to the attention of Dr Townsend by Xavier Azalbert and non-profit BonSens.org attorneys, starting on January 7. A total of nine communications were sent by the above individuals, but none of them were ever shared as ‘Letters to The Editor’ by Dr Townsend in good faith to inform readers of specific potential shortcomings, as is commonly done.
Dr Townsend seemed to forget that bad medical data and publications can do actual patient harm, and kept legitimate and important study criticisms to herself. Instead of taking responsibility and making a leadership decision, she passed the buck to a Committee on Publication Ethics, delaying the needed retraction.
Appallingly, it took 234 days (~7 months, from the January 2 publication to August 26) for Dr Townsend’s Journal of Biomedicine and Pharmacotherapy to retract the ‘unreliable’ article. By that point, untold millions around the world had already been (and continue to be) polluted with outrageously incorrect information about non-existent HCQ deaths.
This raises some questions about Dr Townsend’s duties and responsibilities as the Editor in Chief:
- What efforts were made to correct incorrect headlines and articles published by the lay press, incorrectly frightening patients, pharmacists and physicians, by fuelling false tropes about HCQ?
- What efforts were made to let news organisations know that data from the peer-reviewed publication was under question? (She refers to ‘a number of Letters to the Editor and correspondence from readers‘.)
- What immediate efforts are being made to notify news organisations and/or amplify search engine results regarding the now-retracted publication?
- What funding source/individual paid the $3,490/£2,608 (‘excluding taxes and fees’) publication fee? (Note: reputable academic journals do not charge to publish articles.)
- Does Elsevier’s Journal of Biomedicine and Pharmacotherapy meet certain definitions of what is known as a predatory publisher?
- Was this Editorial Board qualified to review regulatory/drug safety/epidemiology/any other clinical subjects?
- Are the ramifications of this Journal’s publication and its subsequent retraction known to the University of South Carolina administration, co-faculty, and whichever body adjudicates its faculty Code of Ethics & Standards of Practice?
- This isn’t the first time Townsend has needed to retract articles – a normally very rare occurrence for reputable journals. Will Elsevier, which publishes more than 2,700 journals, permit further opining or publishing on clinical subjects by this editorial board? Can the Editor-in-Chief and/or editorial board be trusted to recuse themselves from opining on any topics that are not within their area of expertise?
- What should be done to prevent a reoccurrence of this incident at the University of South Carolina and other taxpayer-funded institutions?
Beyond that, what ramifications/punishments (if any) will occur for other prominent Covid-19 Lancet and New England Journal of Medicine authors/publishers whose articles were also retracted after they were found to be based on so-called ‘unreliable‘ (ie non-existent) databases?
Ethical scientists who believe in truth, transparency, and academic accountability are standing by, waiting for medical and academic justice.
Unethical scientists are also watching this situation unfold, twisting their moustaches, learning about what they could potentially one day get away with.
Journalist Sharyl Attkisson details cancel of hydroxychloroquine, in new book 'Follow the Science'
Attkisson is an Emmy Award winning investigative journalist and the author of "New York Times" best-seller "Stonewalled."
Published: August 28, 2024 11:00pm
Editor's Note: The following is an exclusive excerpt from the new book by investigative journalist Sharyl Attkisson, “Follow the Science: How Big Pharma Misleads, Obscures, and Prevails.” The book, by publisher Harper Collins, is due out Tuesday, Sept. 3.
"If you consume the curated, mainstream medicine and media narrative, you’re probably under the impression that the prescription drug that President Trump touted as a possible game changer against coronavirus – hydroxychloroquine – has been thoroughly 'debunked' and discredited.
"At the height of the Covid panic as politics, money, and medicine intersected – two divergent views of hydroxychloroquine emerged, both of which could not possibly be true at the same time. The first view was the negative one widely reported in the press. The second view you’ve likely heard less about. Rarely has a discussion about choices of medicine been so polluted by political overtones …
"Many right-leaning media figures and independent scientists sided with hydroxychloroquine, while the public health establishment and left-leaning press backed remdesivir. Each accusing the other of ignoring real science.
"I found an informative view from cardiologist Dr. William O’Neill, a medical director at the Henry Ford Health System in Detroit, Michigan, where researchers were studying both remdesivir and hydroxychloroquine and had no known financial stake in the outcome.
“'I’ve never seen science so politicized in forty years of practice,' Dr. O’Neill tells me when I visit with him.
“'Some people in the media are treating hydroxychloroquine as if it’s something that’s being pitched by charlatans [as if] it’s dangerous, debunked, and discredited,' I say to Dr. O’Neill. 'What do you make of that?'" …
"'I think [the negative media narrative on hydroxychloroquine] is very harmful,' Dr. O’Neill tells me. 'President Trump touted it early, and so then the media set out to disprove and discredit it without any regard for science. I think those of us that are actually involved in the scientific endeavor feel that there is some value to it, and it has to be tested.'
"Dr. O’Neill is a world-renowned leader in interventional cardiology, famous for 'pioneering research in new techniques to diagnose and treat heart attacks.' He’s not only an eminent researcher; he’s also a clinician.
"When we first spoke, he’d already prescribed hydroxychloroquine, before the government limited its use, to numerous Covid patients. He tells me he saw improvement in all of them. Real-world, firsthand evidence directly from a scientist involved! On the other hand, he tells me he’s far less impressed by remdesivir.
"'There’s a lot of hype for [remdesivir],' Dr. O’Neill continues. 'I saw the original New England Journal article study and I saw the Lancet study, and to me it’s just like a big ‘Ho-hum. I just don’t see a big benefit.'" …
"A recurring lesson in science, and life in general, is that when the actions of media, government, and public officials seems so contrary to common sense: Follow the Money. You can learn a lot. So, amid the hydroxychloroquine nonsense, I start connecting the dots …
"I go down the list of names on the government’s Covid treatment panel, which dialed back hydroxychloroquine use and promoted newer, more costly remdesivir. I’m looking to see if any of them are connected to companies that make hydroxychloroquine or remdesivir. Ideally, none of the panel members should have links to companies benefiting from their decisions. But that world no longer exists in public health. A second-best option would be for advisors to recuse themselves from decisions involving companies they’re connected to. But that world doesn’t exist either.
"What do I find? About one-third of the government’s Covid treatment advisory panel, or eleven members, reported having links to a drug company. Nine of the eleven named Gilead, the maker of remdesivir! What are the natural odds that so many people chosen for an expert panel on Covid would be related to the company making the treatment they ended up favoring?
"I keep digging.
"Beyond the eleven, I identify nine others, including two of the committee’s three leaders, who also have ties to Gilead but hadn’t disclosed them. Two even served on Gilead’s advisory board! Others were paid consultants or received research support and honoraria from Gilead. They weren’t technically required to fess up those relationships because, under the committee’s special rules, for some reason, panel members don’t have to acknowledge conflicts of interest older than eleven months. As if conflicts of interest somehow become irrelevant after eleven months?
"There’s one more piece of the puzzle I need to find. How many on the same advisory panel report having financial links to remdesivir’s disfavored rival, hydroxychloroquine – a generic drug so cheap that no big drug company will make billions if it works on Covid?
"The answer: zero.
"When I first spoke to Henry Ford Hospital’s Dr. O’Neill, he remained confident that good science would prevail, and studies underway would soon provide definitive answers on hydroxychloroquine’s effectiveness for Covid.
"'I think that it’s just still very early in this disease process that we’re going to learn a lot,' he tells me in late spring of 2020. 'There’s six hundred studies that are being done in the United States right now on Covid to see all sorts of different kinds of infections and combinations. We’re going to be a lot smarter at the end of the summer. So I think what I would just say to everybody, just hold your powder.'
"Not long after, I learn that Dr. O’Neill’s hydroxychloroquine study has been halted by unnamed authorities above his pay grade. It had become pointless, anyway. The FDA’s criticism of hydroxychloroquine had made it impossible to get enough volunteers for the study to move forward. After all, who in their right mind would raise their hand to take part in a trial with medicine the FDA has warned against so publicly?
"'Now people are scared to use [hydroxychloroquine] – without any scientifically valid concern,' Dr. O’Neill tells me when I follow up. 'We’ve talked with our colleagues at the University of Minnesota who are doing a similar study, and at the University of Washington. We’ve treated four hundred patients and haven’t seen a single adverse event. And what’s happening is [that] because of this fake news and fake science, the true scientific efforts are being harmed. Because people now are so worried that they don’t want to enroll in the trials.'
"Dr. O’Neill would later say that 'the saddest part' of all is that we won’t get the definitive scientific answer, either way, to what had been made into a political question.
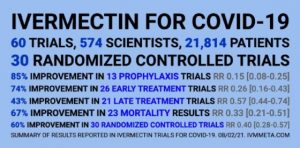
"The government and other vaccine industry allies were soon to arrange for the same unscientific treatment be given to another generic medicine repurposed, 'off-label,' to treat Covid: ivermectin.
The Hydroxychloroquine Crime
More than four years ago, Democrat leaders colluded with the WHO (as part of the wannabe global government) and Big Tech to perpetrate a horrific crime: the denial of access to hydroxychloroquine (HCQ) and other lifesaving COVID-19 treatments. The primary purpose was to legalize fraud-ridden voting by mail and seize power following the 2020 elections. Once in power, the perpetrators were able to cover up this crime even though it is ongoing. The FDA continues to reject HCQ and the even less controversial ivermectin (IVM). Instead, it pushes the harmful and dangerous quasi-vaccine.
The number of direct deaths from COVID-19 has exceeded one million in the U.S. alone. Almost all of these deaths could have been avoided using HCQ- or IVM-based treatment. If not for the unusually mild omicron variant, the death count could be tens of millions.
The effectiveness and safety of HCQ or HCQ-based treatments have not been reasonably questioned on medical grounds since late March 2020. In addition to the rigorous scientific studies led by Prof. Didier Raoult in France, HCQ was the preferred treatment by most doctors treating COVID-19 worldwide by April 2020. The hydroxychloroquine + azithromycin protocol has saved Italy and Spain. Thousands of doctors have attested to its success worldwide. “Sixty-five percent of physicians in new survey would give anti-malaria drugs to their own family to treat COVID-19.” “The top three treatments that doctors reported having prescribed were Azithromycin (58%), Hydroxychloroquine (50%), and Bronchodilators (48%)” And so on. Hardly any practicing physician treating patients with HCQ expressed a negative opinion.

What happened next defies explanation. Obama-Clinton-staffed medical establishment and the WHO, empowered by their Big Tech allies, have practically banned the use of HCQ and other effective COVID-19 treatments of prophylactic measures in the West.
The safety and security departments of Big Tech behemoths were simultaneously suppressing information about Hunter Biden’s laptop and about effective COVID-19 treatments.
Even if the rejection of HCQ could be explained (but not vindicated) by Trump Derangement Syndrome, the rejection of other medicines from IVM to convalescent plasma was not so obviously accounted for.
The aim of the Democrat party was a power-grab. In addition to voting by mail, the pandemic allowed it to hide the already visible dementia of Biden and to blame Trump for pandemic suffering. Another kind of power-grab was also the aim of the WHO. The WHO demanded to be treated as a global FDA, with nations of the world deferring to its decisions on what treatments to use and not to use for COVID-19. Big Tech supported this bizarre demand. After its success, the WHO attempted to enshrine its power in the Pandemic Agreement.
This mass murder by the denial of access to medications became possible because of the migration of communications to the internet and allowing five to seven corporations, selected mainly by the Obama administration, to control it. Regions that did not rely on the internet much, such as Africa, or where internet communications were not entirely under the same Big Tech control, including Asia, had much lower COVID-19 death rates.
Big Tech is capable of such crimes because of how it operates. Both pompous executives and little operatives making changes in its databases stay far removed from the suffering and death of the people caused by their actions.
Too much of the blame is directed at Dr. Fauci and “Big Pharma.” Dr. Fauci was likely misled by the assault on HCQ, which was conducted through Big Tech manipulations. The medical establishment probably had too much of the old guard linked to the Clintons. Congressional Democrats preserved it. For example, they forced the resignation of Trump-appointed CDC director Dr. Brenda Fitzgerald by false accusations of conflicts of interest.
But even in this environment, Fauci could not suppress HCQ. It was already widely used in April 2020. Physicians did not require permission from Fauci or the FDA. Big Pharma played a secondary role. Yes, Gilead has added to the defamation of HCQ to promote its anti-kidney Remdesivir. However, it could do so only because it had political support.
None of the guilty parties has publicly changed its position or admitted that it was wrong. Most of them are in a position of power. The FDA still denies the effectiveness of IVM for COVID-19, even after it settled a lawsuit about its earlier false claims.
We could not discuss the suppression of COVID-19 treatments in 2020 because Big Tech suppressed such discussions and because it was hard to believe.
We could not discuss it after the Biden regime came to power because congressional Democrats were conducting official investigations against doctors defending HCQ for COVID-19. HCQ-based treatment is associated with Donald Trump, and the Biden administration has been targeting organized Trump-supporters as violent extremists.
Supporting the use of hydroxychloroquine for COVID-19 was cited as aggravating evidence against Dr. Simone Gold, who was among other people admitted by the police into the Capitol on Jan 6: “On January 5 [sic], GOLD gave a speech in support of the use of hydroxychloroquine and against COVID-19 lockdowns.” She was arrested on January 18, 2020.
This mass murder, committed by denying access to life-saving treatments during the pandemic, cannot be forgiven or forgotten.
Hydroxychloroquine Reduces COVID-19 Mortality, Study Finds
Researchers examined records from 352 adults hospitalized in AZ Groeninge Hospital in Kortrijk, Belgium.
10/9/2023
People who took hydroxychloroquine in combination with another drug while hospitalized with COVID-19 were less likely to die than those who didn't, according to a new study.
Hydroxychloroquine, which is widely used against malaria and arthritis, was given to hundreds of patients hospitalized with COVID-19 in Belgium. Thousands of others didn't receive the drug.
Researchers examined records from 352 adults hospitalized in AZ Groeninge Hospital in Kortrijk, Belgium. All patients tested positive for COVID-19 or had results from CT scans that suggested COVID-19 was present. Patients received hydroxychloroquine alone or with azithromycin, an antibiotic. They were scanned before and after treatment.
Researchers compared the results of the record analysis with a control group of 3,533 people hospitalized across Belgium with COVID-19 from March 14, 2020, to May 24, 2020. The people didn't receive hydroxychloroquine but did receive standard of care.
Twenty-eight days following the diagnosis of COVID-19, 59 people treated with hydroxychloroquine had died. The mortality percentage, or 16.7 percent, was lower than the 25.9 percentage in the control group.
Researchers found patients who received hydroxychloroquine were more likely to survive even after adjusting for age and other factors.
How Quercetin Works Like Hydroxychloroquine to Stop Viruses
"Our study suggests that, despite the controversy surrounding its use, treatment with hydroxychloroquine and azithromycin remains a viable option," Dr. Gert Meeus, a nephrologist with AZ Groeninge Hospital, and other researchers wrote.
The study was published by the journal New Microbes and New Infections. Limitations include the retrospective nature of the study and differences between the treatment and control groups, including the former being younger on average. Authors declared no conflicts of interest or funding.
The research adds to a mixed dataset on hydroxychloroquine against COVID-19.
Some other studies have found that hydroxychloroquine recipients were less likely to die, including a study that analyzed records from a health system in Michigan. Many of the positive findings concerned hydroxychloroquine in combination with azithromycin.
Others have found little or no evidence that hydroxychloroquine affects COVID-19, including a U.S.-government funded study across 34 hospitals.
Multiple studies on hydroxychloroquine and COVID-19 have been retracted.
Hydroxychloroquine is approved by the U.S. Food and Drug Administration but the agency has warned since mid-2020 against using it for COVID-19. Belgian regulators rescinded authorization for hydroxychloroquine for COVID-19 in June 2020.
Dosage Issue?
Hydroxychloroquine proponents say that the amount of the drug, and when it's given, is key to properly studying how it affects COVID-19.
Dr. Meeus and the other Belgian researchers acknowledged clinical trials that did not find a benefit for hydroxychloroquine, as well as some observational studies. Other observational papers have suggested hydroxychloroquine is effective.
"A potential explanation for the discrepancy between the results in the observational trials and the large randomized trials may be the use of a different dose of hydroxychloroquine," they said.
The researchers started with 400 milligrams, two times a day, on day one. That was followed by 200 milligrams a day for five days, in line with national guidelines.
In the clinical trials that found no benefit, patients received four times as much hydroxychloroquine.
"Our treatment was lower and also used the antibiotic azithromycin. This double treatment is a possible explanation for why we found positive effects, but other studies did not," Dr. Meeus told Doorbraak.
Peter Horby, a spokesman for one of the trials, told The Epoch Times previously that the dosage amounts were "carefully selected" and "designed to achieve the concentrations needed to inhibit the virus as quickly and safely as possible."
Dr. Meeus told Doorbraak that further research needs to be done on the drug, or HCQ, but that it very well could be beneficial.
"HCQ is not a panacea, and of course, further research needs to be done. After all, you can't just conclude from an observational study like ours whether something works or not," he said. "But look, we have followed the protocol as it was originally prescribed in Belgium. A study ... also showed in early 2020 that HCQ did lead to lower mortality. If the results of our study confirm this again, we think it is very plausible that the drug has helped quite a few patients."
A Review of Helpful Antiviral Strategies Dr Mercola April 19 2020
STORY AT-A-GLANCE
- Initial predictions called for 2.2 million COVID-19 deaths in the U.S. alone. According to the latest models, an estimated 60,000 Americans may die from COVID-19 complications
- Some doctors are promoting the use of the antimalarial drug hydroxychloroquine combined with azithromycin for seriously ill COVID-19 patients. Apparently, many are seeing good results, although not universally. Some Swedish hospitals have stopped using chloroquine due to severe side effects in some patients
- Northwell Health, New York's largest health care provider, is using vitamin C at its hospitals in conjunction with hydroxychloroquine and azithromycin
- Some doctors have noted their patients’ symptoms have more in common with altitude sickness than pneumonia. In the final analysis, it may turn out that ventilators are inappropriate for a majority of patients. A better alternative may actually be hyperbaric oxygen therapy
- Preventive methods you can use at home include taking vitamin C to bowel tolerance; zinc, vitamin B1 and melatonin supplementation; nebulized hydrogen peroxide; ozone therapy and nitric oxide boosting exercise
In this interview, recorded April 7, 2020, Dr. Andrew Saul, editor-in-chief of the Orthomolecular Medicine News Service, brings us new updates and insights into the COVID-19 pandemic.
Since our March 17, 2020, interview, which focused on the use of vitamin C, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, made the prediction that SARS-Cov-2 would kill anywhere from 100,000 to 240,000 Americans,1 which is still far less than the original prediction of 2.2 million.2
However, even that prediction has since been revised downward. April 8, 2020, a new model referred to as the Murray Model3 predicts COVID-19 will kill 60,000 in the U.S. by August.4 There's no doubt in my mind that there will be more deaths from the financial collapse than there will be from the actual infection. So, it's a sad state of affairs. As noted by Saul:
"Folks need to remember that in any given year, influenza escalating to pneumonia is a killer. And in any given year, there's around 40,000 to 65,000 deaths, depending who you listen to, from pneumonia.
This is an awful lot of people dying every year. COVID-19 is a serious disease, but it's not worth shutting down the world for. The stress from that is going to be a killer …
The people who die from COVID-19 are dying basically from SARS, Severe Acute Respiratory Syndrome, or pneumonia. So, it doesn't really matter what virus does that. It matters if you die or not.
Many people are going to get COVID-19, and they're going to have a mild case. And, for those who have a typical case, they're going to have a miserable flu. They're going to be sick as a dog for a couple of weeks.
Well, welcome to humanity, because how many times have we all had a miserable flu in our lifetimes? Those who are really at risk from COVID-19 usually have multiple pre-existing health problems, or they have a demonstrably poor lifestyle.
They're overweight or they're smoking, or they have an impaired immune system, or they're elderly. And if you have a combination of those, anything can take that person out. So, we have to have perspective here."
Google, Facebook Censor Real Data
Unfortunately, if you're still using Google or social media platforms like Facebook, you're unlikely to locate sensible information about how to protect yourself from COVID-19.
I believe suppressing access to the truth — the information you need to upregulate your innate immune system — is part of the plan to control the discussion about treatment options. Clearly, Fauci is promoting a pharmaceutical agenda when he says there's nothing anyone can do until there's a vaccine or antiviral drug available. Saul provides the following real-world example:
"This is something you can verify with your own Facebook account. Try this little experiment. If you post the meme I have at DoctorYourself.com on Facebook, it will immediately be blocked.
Here's what the poster says: 'Dr. Enqiang Mao, who is chief of emergency medical service at Ruijan hospital in Shanghai, China, treated 50 patients with high dose intravenous vitamin C. They had moderate to severe COVID. 50 out of 50 recovered. There were no fatalities.'
This is a report from a senior physician, right from China, to my contact in China, Dr. Richard Chang, who is a board-certified himself and a Chinese-American, right there, reporting in firsthand. And this is labeled false news, fake news. This is demonstrably oppressive."
The good news is Chang is presenting his evidence before the National Institutes of Health. "I've seen his PowerPoint," Saul says. "He's going to run down why vitamin C is an antiviral, and how it can be used, and what doctors are doing."
Aside from Mao, Dr. Zhiyong Peng, chief physician at Zhongnan Hospital, who is doing a major COVID-19 trial in Wuhan City, China, has stated that intravenous vitamin C is successful. "The number of new cases of COVID in China is very low, it's gone way down, almost to the vanishing point," Saul says. "Yet this information, somehow, is not on the news. And this is the very thing America and the rest of the world so needs to know now."
Immune-Boosting Supplementation Regimen
Some New York hospitals are using vitamin C, though. A Northwell Health spokesperson has reportedly confirmed that vitamin C treatment is being "widely used" against coronavirus within the 23-hospital system.
According to Dr. Andrew G. Weber, a pulmonologist and critical-care specialist affiliated with two Northwell Health facilities on Long Island, vitamin C is being used in conjunction with the antimalarial drug hydroxychloroquine and the antibiotic azithromycin, which have also shown promise in coronavirus treatment.5 Saul notes:
"Northwell, which is the largest health care provider chain in New York state, [has] over 20 hospitals. It's difficult to get information out of them, but to their credit, their spokesperson has announced that vitamin C is being used. And Weber … has reported that the vitamin C works. He said, basically, as close as I can quote him, 'It's not getting more publicity because it's not a sexy drug.' I love that …
If you have vitamin C for prevention, you are much less likely to have a bad case of any kind of viral infection, including COVID-19. Doesn't mean you won't get it; it means that your immune system will be able to handle it, and that's what your immune system does …
In fact, people now are being told if they can manage this at home, [then] please stay home. Leave the hospital beds for those who really need them, and reduce risk of infection.
Remember, a hospital, by definition, is where we have our very sickest people with the greatest load of viruses and drug-resistant bacteria that you'll ever find … We don't live in a bubble, we live in a world of viruses, and they're constantly mutating, and they're constantly developing …
So, for prevention, the Orthomolecular Medicine News Service Editorial Review Board and the Japanese College of Intravenous Therapy both recommend 3,000 milligrams (mg) of vitamin C a day in divided doses, 400 mg of magnesium … 20 mg of zinc … 100 micrograms (mcg) of selenium … and 5,000 units of vitamin D, scaling down to 2,000 units of vitamin D a day after the first week.
That is a big difference. So, between the vitamin D and the vitamin C, we have something that will strengthen the immune system. When a person is in hospital, they are less likely to have access to supplements, at a very time when they're going to need them more.
This is why we have to push, and the only way to do that is for the family to get in there and make it happen. More and more doctors are willing to do it because of the studies … in New York … So, the cat's out of the bag … and it's not going to go back in. There is a precedent. Just say to your doctor, 'I want you to do what they're doing in New York' …
What we should learn from history is "have a strong immune system and you will survive." This is the way it works. And the emphasis now is on scaring people, and actually telling them in the media, "Don't take vitamin C, it won't help you. Don't take extra vitamin D, you don't need it. There's nothing you can do to build your immune system."
You'll actually see this on some news reports, and some newspapers. But, you'll also see others that are reporting that it's working in China and other parts of the world."
Zinc With Hydroxychloroquine
Some doctors are promoting the use of the antimalarial drug hydroxychloroquine (Plaquenil) combined with azithromycin (Z-Pak) for seriously ill COVID-19 patients. Apparently, many are seeing good results, although not universally.
According to Newsweek, some Swedish hospitals have stopped using chloroquine due to severe side effects in some patients.6 That said, it appears one of the reason quinine drugs work is because it allows zinc to enter the cells. Saul comments on the use of hydroxychloroquine saying:
"I think if you can use a nutrient with a drug, you get better results than if you use the drug alone. Dr. Abram Hoffer, who was my personal mentor … said, 'Sometimes you need a drug. Sometimes the drug will get you that immediate result that you've got to have, but you have to have nutrition if you want it to stick.'
So, if you use medication and the nutrient, you're going to do better than if you use the medication alone … If the drug will help get the zinc to where it needs to go, that just makes good sense to me."
Since the drug is now being rationed to those who need it most, you'd be wise to take zinc preventively. Your body only needs a small amount of it, and knows exactly what to do with it. Your immune system, for example, requires it to function. The elderly, who tend to eat less and eat less wholesomely, have a greater need for zinc supplementation.
"This is in every nutrition textbook ever written," Saul says. "So, what we want to do right now is tell people, 'Don't worry about the drug unless you really need it. It'll be at the hospital pharmacy. But for the rest of us, let's stay out of the hospital by taking a step so we won't need the drug.'
It's not about avoiding doctors; it's about not needing them. And that means you have to get on the wagon here. We have to do this every day. We have to be sure we take our supplements and eat a good diet, and avoid the junk and continue to get our fresh air and exercise."
Ventilators May Do More Harm Than Good
In recent days, we're seeing more and more reports of doctors saying the use of ventilators may be misguided.7 According to Business Insider,8 80% of COVID-19 patients in New York City who are placed on ventilators die, causing some doctors to question their use. As reported by STAT News:9
"What's driving this reassessment is a baffling observation about Covid-19: Many patients have blood oxygen levels so low they should be dead. But they're not gasping for air, their hearts aren't racing, and their brains show no signs of blinking off from lack of oxygen.
That is making critical care physicians suspect that blood levels of oxygen, which for decades have driven decisions about breathing support for patients with pneumonia and acute respiratory distress, might be misleading them about how to care for those with Covid-19.
In particular, more and more are concerned about the use of intubation and mechanical ventilators. They argue that more patients could receive simpler, noninvasive respiratory support, such as the breathing masks used in sleep apnea, at least to start with and maybe for the duration of the illness."
Some doctors have noted their patients' symptoms have more in common with altitude sickness than pneumonia.10 This situation highlights the problems inherent with strategic standard of care. We thought we had a serious ventilator shortage and industries such as the auto industry redirected their manufacturing capacity to making ventilators.
In the final analysis, it may turn out that ventilators are inappropriate for a majority of patients. A far better alternative may actually be hyperbaric oxygen therapy.
"Making the oxygen available in a way that's appropriate to the severity of the patient is the answer," Saul says. "We have to remember that our body is singularly good at taking in oxygen or we wouldn't be here. And our lungs have a huge amount of absorptive space. I mean, that's what they do. It's just an extraordinary system that we have.
Oxygen goes in by diffusion. You don't push it in; the body sucks it in because if you have more oxygen outside than you do inside, it just goes through. All you do is give a lot of absorptive surface. And if you flattened out all the little alveoli in the lungs, you'd have an enormous area …
So, by providing the oxygen and then see if the body will take it up, you've made the first step. That can be done preventively by fresh air and exercise and going out and playing …
If somebody needs more oxygen, and you want to give them a little pressure, if that makes the patient better, then you do it. But the idea that you've got to ram this oxygen like a supercharger on a Mustang is, I think, a little bit, shall we say, industry friendly …
[The alveoli] are tiny, tiny little sacks. They have some of the thinnest little membranes you've ever seen. Look at them under a microscope. They're very delicate. So, the last thing you want to do is add injury to insult."
Hydrogen Peroxide Therapy
Saul, along with Dr. Thomas Levy, recommend nebulized hydrogen peroxide therapy. Similarly, Dr. Robert Rowen has published a commentary11 about the use of ozone therapy against SARS-CoV-2 infection. Both of these treatment alternatives are inexpensive and safe, and could be administered at home.
One point I want to stress after looking more deeply into this is that you may want to be careful about using regular 3% hydrogen peroxide, as they use proprietary stabilizers. By law, they're not required to disclose those chemicals. So, ideally, you'd want to use food grade hydrogen peroxide and carefully dilute it to a 3% concentration.
What to Do if You're Feeling Under the Weather
So, to recap, what can you do if you're suddenly feeling under the weather and suspect a viral infection? Saul recommends taking vitamin C to bowel tolerance.
"Take enough C to be symptom free, whatever the amount might be. Dr. Cathcart would say take vitamin C to bowel tolerance, and that's exactly what you think it means. The sicker you are, the more you hold. So, if you are really facing an influenza outbreak, you'll hold a lot of C before you get to bowel tolerance.
This is something that everyone can do at home. My grandchildren can do this. When they get sick, they manage their own case by taking vitamin C until they get to bowel tolerance. Use whatever kind of vitamin C you can afford … [and] take enough C to be symptom free.
The more frequently you can take the vitamin C, the better off [you'll be]. Vitamin C being water soluble is constantly lost … The more often you take it, the better results you will have, and you will need less to do so.
So, taking a small amount of vitamin C every half-hour is actually much better than taking a large amount of C twice a day. And taking a large amount of C twice a day is better than taking a huge amount of C every other day. So, the more often you take it, the friendlier it is for your body."
For acute infection, you may need to increase your dosage somewhat beyond bowel tolerance. Keep in mind that taking it more frequently, such as every half-hour, will allow you to take more before you hit bowel tolerance. Other alternatives include taking a liposomal vitamin C or getting an IV infusion of vitamin C. Liposomal vitamin C can achieve intracellular levels very similar to IV vitamin C at a fraction of the cost and inconvenience.
B Vitamins (Thiamine)
Thiamine (vitamin B1) is also important, and works synergistically with vitamin C. Any infection increases your body's need for thiamine. You can read more about this in "Vitamin B1 Is Vital to Protect Against Infectious Disease."
The recommended daily allowance for thiamine is well below 2 mg. For acute illness or short-term prevention, Saul suggests taking 50 mg to 100 mg of thiamine per day, ideally in divided doses.
"Thiamine is the vitamin that smells funny," he says. "When you open the bottle of your multiple vitamin, or your B complex, that smell is thiamine. So, when your urine smells like thiamine, you're probably getting more than you need, but that's not a problem.
Thiamine is safe, and you can excrete that. The excretion is an indicator of saturation. Thiamine, really, is best taken with the entire B complex. The B complex vitamins work better together.
For prevention, most people will get a B complex, B50 … Generally speaking, what I would tell people to do is take a look at the RDA, and you can do that on the internet in seconds, and take more than that. A B complex is this cheapest and safest way to do that."
Melatonin for COVID-19
Another strategy that appears useful against both bacterial and viral infections is hormone melatonin. I review this in greater depth in "Melatonin for Sepsis." Saul comments:
"Melatonin is a wonderful thing, because the safety studies are very encouraging. If you want to hurt yourself, melatonin will not do the job … Melatonin is inexpensive, it's non-prescription and, obviously, something that safe deserves a try … And a little bit of melatonin can go a long way.
The older you get, the less you make. Now, if you keep your bedroom dark at night, you will make more melatonin. I'm about to impart a piece of wisdom that makes me very unpopular very quickly with a large number of people, and that is if you go to bed early, you will make more melatonin, and you will sleep better.
If you go to bed at 7:30 or 8:00 o'clock at night, you will have a far better sleep than if you go to bed later, even if you have the same number of hours. The old adage is, each hour of sleep before midnight is worth two hours of sleep after midnight. There's something to that."
Nitric Oxide Helps Inhibit Viral Replication
Another strategy worth mentioning is nitric oxide, which appears to inhibit viral replication. To boost nitric oxide, you could use precursors such as arginine or citrulline, but exercise and near-infrared radiation (such as a near-infrared sauna) will also do the trick.
"Exercise is absolutely crucial. I'm so big on that, and I would like to underscore that this is something that doesn't cost a dime," Saul says. "What is missing from most discussions on COVID-19 is an appreciation of how far we have let ourselves go. We've been eating crummy food for a long time.
We've been doing behaviors for a long time that don't work. And sooner or later, the body is going to be weakened by that. Too much of the wrong thing, not enough for the right thing, and the immune system is going to be weak. And viruses, unfortunately, to put it very coldly, will thin the herd.
This is the way nature works … Now, this is a very harsh lesson from nature, but we would do well to learn it. If we let ourselves go, as my mother would say, 'If you do this wrong, and you know it, don't come crying to me afterwards.' We have to take responsibility, and right now the COVID-19 epidemic is pointing that out in a very, very strong way.
It is most unpleasant to see this, but bearing in mind that we are not a healthy nation, we have to immediately take steps to become one, or there will be another virus, because this is not the first, and it is not the last … It just makes my day when I learn about people that … are not watching the news, they're going out and they're getting well."
Sources and References
- 1 CNN March 31, 2020
- 2 The Intercept March 17, 2020
- 3 IHME April 2, 2020
- 4 CNN April 8, 2020
- 5 New York Post March 24, 2020
- 6 Newsweek April 6, 2020
- 7 Medscape April 6, 2020
- 8 Business Insider April 9, 2020
- 9, 10 STAT News April 8, 2020
- 11 Journal of Infectious Diseases and Epidemiology, A Plausible “Penny” Costing Effective Treatment for Coronavirus — Ozone Therapy

Search our Site...



