
Ivermectin Prescriptions Soaring In England
The latest on this little old medicine with a variety of uses
Tess Lawrie MBBCh PhD
July 14th 2026
I have reported on ivermectin in several substack articles. Here are some:
April 2021 ‘IVERMECTIN evidence pack was delivered to UK Prime Minister Mr. Boris Johnson’
March 2022 ‘A Letter to Dr Andrew Hill. Ivermectin: The Truth vs Goliath’
July 2022 ‘Ivermectin works – just not for Big Pharma’
January 2023 ‘Can cancer really be cured with ivermectin and other safe, old treatments?’
February 2023 ‘Why Are They So Desperate To Keep Little Old Ivermectin From You?’
March 2023 ‘Ivermectin and cancer: reserved for horses?’
July 2023 ‘#MyIVMStory for World Ivermectin Day’
January 2024 ‘Retired General Practitioner finds ivermectin useful to treat shingles’
August 2024 ‘Is ivermectin really a genocidal tool of the globalists?’
August 2024 ‘Exploring Ivermectin’s Impact on Fertility in Africa’
September 2024 ‘Coming full circle with ivermectin and ‘the science’’
December 2024 ‘Ivermectin Attacks continue’.
The campaign to get ivermectin adopted as a treatment for ‘covid-19’ symptoms started way back in mid-2020. The pushback from governments, institutions and media was relentless. So, you may wonder, why I have now posted these links. Well, I have some good news!
In the last substack above, there was a chart showing how officially prescribed ivermectin prescriptions had risen markedly from mid-2023 in the UK. There was an astonishing 11x increase over early 2020. The source I used was openprescribing.net. Here is what the chart of official NHS prescriptions looks like now, with the latest data up to the end of March this year.
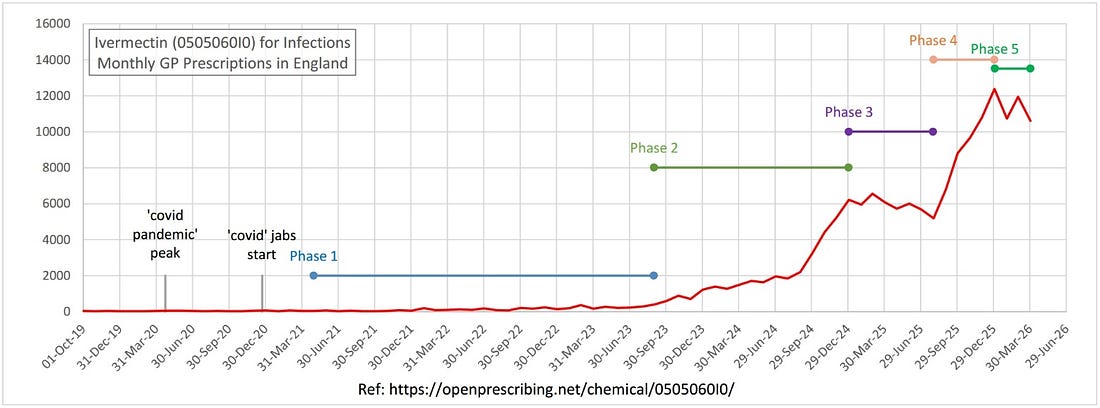
What averaged 33 prescriptions per month in 2020 became 372 prescriptions in 2023, 2,200 prescriptions in October 2024 and is now 11,000 prescriptions! This represents an over 300-fold increase!
The chart may be split into different phases to show how suppressed treatments break through institutional resistance. This is apparently a textbook case – a diffusion curve with a capacity plateau in the middle. The characteristics are:
Innovation (2021–2022): A handful of doctors and patients, operating against official guidance.
Early adoption (2023): The private prescriber network builds, word-of-mouth spreads.
Capacity ceiling (early 2025): The existing network reaches an intermediate capacity limit.
Late adoption (late 2025): Mainstream GPs enter, supported by a US policy shift and less perceived risk.
Normalisation (2026 onwards): Established as part of primary care prescribing.
The World Council for Health, BIRD and other organisations and individuals have been tirelessly promoting this cheap, safe and effective pharmaceutical – and not just for ‘covid-19’. It remains very useful for eliminating parasites, and is increasingly selected by individuals with cancer as part of their treatment program. It is encouraging to see how traction has been gained over nearly six years. A huge amount of patience and persistence was necessary. Let’s look at each phase in turn.
Phase 1 (May 2021 to Aug 2023)
This is sometimes referred to as the ‘whispering’ phase. There was maximum suppression, the ‘horse paste’ smear, scare tactics etc. The spread was slow, by word-of-mouth. Some doctors were convinced by the literature from the FLCCC and BIRD initiative campaigns. They took career risks. There were ‘long covid’ and jab adverse reaction sufferers who were dissatisfied with NHS treatments that benefitted.
Phase 2 (Sep 2023 to Dec 2024)
The ‘covid’ inquiry (however farcical) showed up the ‘pandemic’ response and ‘trust the science’ was exposed. The ‘long covid’ and chronic jab adverse reactions were prolonged without effective NHS treatment.
Every successful patient who adopted ivermectin become a referral source for five more patients. Similarly, doctors prescribing ivermectin without GMC sanction encouraged other doctors to do likewise. Pharmacy resistance reduced as more prescriptions were received. The effect of the US election with Robert Kennedy Jr. and MAHA brought the benefits of ivermectin into the public eye.
There was a cost reduction from £348, including a sudden halving in May 2024 from £170 to £82. At 5,000 prescriptions per month, it was becoming normalised and no longer easy to demonise.
Phase 3 (Jan 2025 to July 2025)
Sometimes called ‘saturation’, the system reached an intermediate ceiling. New patients may have been entering at the same rate as those finishing their treatments. Doctors may still have had some caution about prescribing more in case it triggered a GMC response, particularly as there were delays in the US appointing Robert Kennedy Jr. and making policy changes.
Phase 4 (Aug 2025 to Jan 2026)
This marks the real lift-off. The US MAHA agenda began implementation and CDC’s position on vaccines and autism changed. UK doctors, once hesitant, could now feel supported. The GMC was effectively neutralised by US events, so mainstream NHS doctors begin prescribing. The media were no longer publishing scare-mongering stories on ivermectin. They had been rumbled!
Phase 5 (Jan 2026 to present)
This now appears to be a normalising period. New patients are entering at the same rate as those finishing their courses. The January peak is a typical high-prescribing month. From October 2025, the cost of treatment seems to nearly double again (£91 to £164) – although this is way lower than alternative (and ineffective) treatments.
Summary
This is where we are now: the same NHS that spent 2021 telling patients ivermectin was dangerous horse paste is now quietly dispensing it at a rate of over 10,000 prescriptions a month. This is because of sterling work of WCH, BIRD, FLCCC and others to publicise its benefits, and because of American political pressure that made the suppression unsustainable. The data doesn’t lie – even when the institutions do.
Finally, this analysis relates to officially-prescribed ivermectin. An unquantifiable amount of ivermectin was – and still is – purchased privately in large batches at 1/100th the cost of NHS prescriptions. The experiences of those who have used it will have filtered through to NHS patients. Word of mouth of its effectiveness for a variety of applications may now be the most powerful influence of all!
Ivermectin Use Through the Roof
Anti-Metastatic Effects Gain World-Wide Recognition

Ivermectin can be manufactured for about 3 cents per pill, yet numerous and growing reports are emerging that it is effective against cancer. Not just cancer in the early stages. The evidence is accumulating that Ivermectin is effective against metastatic disease - terminal cancer. Stage 4 cancers.

This article suggests that high-dose Ivermectin shrinks cancer metastases.

To my knowledge, this is a first. There are NO drugs approved by the FDA to shrink cancer metastases.
This next article describes a case report of a patient recovering from Stage 4 colon cancer with the use of Ivermectin. He had sent home to die by his Oncologist.

Indeed, Sloan Kettering trained cancer researcher, Dr. Kathleen Ruddy was so impressed with Ivermectin’s effectiveness in terminal cancer patients that she helped begin a multi-center clinical trial to prospectively study Ivermectin in this regard.

When I began writing about Ivermectin in the book Ivermectin for the World, which was published on June 15, 2021, Ivermectin prescribing was but a blip on the radar. I wrote this in the book’s Postscript:
In closing, allow me to share something that is never mentioned enough. Many may not know this, but what is important here is one thing: Repurposed Drug Cocktails work against viruses - And Repurposed Drug Cocktails work against Terminal Cancer. And they work spectacularly well.
The other important thing to remember is this: Big Pharma controls Big Regulators and can manipulate the studies to show anything they wish.
And Big Pharma will always protect their Chemotherapy Industry. It is worth billions. You can expect them and their brethren, the FDA, CDC, and NIH to ALWAYS be opposed to safe, cheap, and effective repurposed drug cocktails for cancer regardless of whether they work.
Finally, Dr. Tess Lawrie recently wrote an article on Ivermectin and the rapid rise in prescriptions measured in the UK.

In this article, Tess brings up the recent accusations that Ivermectin can harm fertility, and that it is somehow being used as an agent to depopulate. Is this true?
The short answer is that following the billions of doses used to treat River Blindness, fertility rates actually increased. Go figure.
The longer answer circles back around to what I wrote in my 2021 book:
And Big Pharma will always protect their Chemotherapy Industry. It is worth billions. You can expect them and their brethren, the FDA, CDC, and NIH to ALWAYS be opposed to safe, cheap, and effective repurposed drug cocktails for cancer regardless of whether they work.
Ivermectin Fact Sheet
Dr Mary Talley Bowden
Safety:
- Approved for human use in 1987.
- Has been administered over 4 billion times around the world.
Day 8 is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
- On the WHO’s list of essential medications.
- Won a nobel prize for its impact in global health
- Not considered toxic to liver, kidneys or lungs (LiverTox, NephroTox and
PneumoTox databases)
- 2 RCTs showing no adverse events in using ivermectin to treat COVID at
0.6mg/kg/day.
- 2020 systematic review and meta analysis in Journal of Antimicrobial
Chemotherapy, Navarro et al. Looked at 6 studies and showed no increase in
adverse events with doses higher than 0.4mg/kg/day (up to 0.8mg/kg/day)
- Over 10 years of studies showing ivermectin inhibits the replication of at least a
dozen RNA viruses.
- No drugs with absolute contraindications. Rare reports of increased INR when
taken with warfarin.
- Pregnancy class C. Use with caution, weigh risks versus benefit. Not studied
in pregnant women.
- Does not cross blood-brain barrier.
- Metabolized by the liver. CY3PA4
- Half life of 18 hours. Peak concentration in 4 hours.
- Side effects listed in the patient information packet: Headache, dizziness, muscle pain, nausea, or diarrhea may occur. (0.9 - 2.8%)
- Study of 963 patients (treated for parasites): tachycardia (3.5%), peripheral edema (3.2%), eosinophilia (3%), facial edema (1.2%), orthostatic hypotension (1.1%), hemoglobin increase (1%)
- FDA approved to treat strongyloidiasis and river blindness (onchocerciasis). Off-label for blepharitis, head lice, scabies, rosacea.
- Not studied in children weighing less than 15kg.
- LD50 is a benchmark number used to gauge a medication’s toxicity. The median LD50 of ivermectin ranges from 11.6mg/kg - 87.2mg/kg in adult mice and rats. The doses used for COVID range from 0.2mg/kg - 0.6mg/kg (19 - 436x the treatment dose.)
- 14 week daily dose of 0.4mg/kg had no adverse effects in rats. A 14 week daily dose of 0.5mg/kg daily had no adverse effects in dogs.
Efficacy:
Real-time meta-analysis of studies looking at ivermectin for COVID:
- Currently up to 105 studies, 52 RCTs Significantly lower risk is seen for mortality, ventilation, ICU admission, hospitalization, recovery, cases, and viral clearance. All remain significant for higher quality studies. 64 studies from 58 independent teams in 27 different countries show significant improvements.
- Meta analysis using the most serious outcome shows 61% [50‑69%] and 85% [77‑90%] lower risk for early treatment and prophylaxis, with similar results for higher quality studies, primary outcomes, peer-reviewed studies, and for RCTs.
- Results are very robust — in worst case exclusion sensitivity analysis 63 of 105 studies must be excluded to avoid finding statistically significant efficacy.
- Late treatment shows 43% decrease in mortality, 47% decrease in intubation
https://t.me/LauraAbolichannel
Fifth Circuit Rebukes FDA for Banning Ivermectin for Covid-19
The U.S. Court of Appeals for the Fifth Circuit issued a unanimous three-judge decision on September 1, 2023, holding that the Federal Drug Administration (FDA) overstepped its statutory authority by attempting to ban using ivermectin to treat COVID-19. In Apter v. Department of Health and Human Services, court concluded, “FDA is not a physician. It has authority to inform, announce, and apprise—but not to endorse, denounce, or advise.”
Writing for the three-judge panel, Circuit Judge Don R. Willett began the court’s opinion by citing the strident nature of the FDA’s opposition to ivermectin as a COVID-19 treatment. Willett opened his opinion as follows:
“You are not a horse.”
Or so the Food and Drug Administration (“FDA”) alerted millions of Americans via social media, midway through the COVID-19 pandemic. The agency had discerned that some people were treating their symptoms using the animal version of a drug called ivermectin. FDA decided to target the practice via the “horse” message—and others like it. The messaging traveled widely across legacy and online media. Left unmentioned in most of that messaging: ivermectin also comes in a human version. And while the human version of ivermectin is not FDA-approved to treat the coronavirus, some people were using it off-label for that purpose.
The case involved three physicians, Robert L. Apter, Mary Talley Bowden, and Paul E. Marik, each of whom jeopardized his or her professional career by prescribing ivermectin for COVID-19 in defiance of the FDA warnings. Apter and Bowden claim to have treated or consulted more than 9,000 COVID-19 patients, with each experiencing a 99 percent survival rate, despite regularly prescribing them ivermectin off-label as a treatment.
Under FDA regulations, any licensed physician may prescribe “off label” any medication the FDA has approved, even if the FDA has not approved the medication for the illness for which the physician is writing the prescription. In 1996, the FDA approved ivermectin to treat in humans parasitic diseases caused by parasites. For daring to ignore the FDA’s vociferous public relations campaign demonizing the use of ivermectin to treat COVID-19, the Courthouse News Service reported “a major Houston hospital system forced Talley Bowden to resign her privileges; Apter was referred to physician regulatory boards of Arizona and Washington state for discipline; Marik was forced to resign from his post at Eastern Virginia Medical School, where he was a medical professor and chief of pulmonary and critical care.” Pharmacies across the nation quit filling prescriptions for ivermectin to treat COVID-19 based solely upon the FDA’s stridently broadcast admonitions not to do so.
Marik joined Pierre Kory, M.D., MPA, co-author of the 2023 book The War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the Pandemic, as one of the critical care specialists co-founding the Front Line COVID-19 Critical Care Alliance (FLCCC), the 501(c)3 organization that brought the case to federal court. In federal court, FLCCC attorneys argued that the FDA’s messaging interfered with their individual “ability to exercise professional medical judgment in practicing medicine.” The doctors also alleged that the FDA’s internet posts on social media demonizing the use of ivermectin to treat COVID-19 “harmed their reputations.”
The Fifth Circuit’s decision does not mean that the FDA now approves of ivermectin to treat COVID-19. But by ruling that Apter et al. had standing to bring the case, the Fifth Circuit’s admonition that the FDA had overstepped its legislative authorization was loud and clear. The Fifth Circuit reversed the district court’s ruling that FLCCC lacked standing to bring the case against the FDA, remanding the case back to the district court.
Still, the decision could not be more important, given that the World Health Organization (WHO) Director-General Dr. Tedros Adhanom Ghebreyesus is already warning that there are “concerning trends for COVID-19 ahead of the winter season in the northern hemisphere,” including increased ICU admissions and hospitalization in Europe. CNN sounded the alarm over a “highly mutated new variant of the virus,” BA.2.86. The newest version is nicknamed “Pirola” and “has more than 30 amino acid changes to its spike protein compared with its next closest ancestor, the BA.2 subvariant of Omicron, according to Dr. Jesse Bloom, who studies viral evolution at the Fred Hutchinson Cancer Center in Seattle.”
In the War on Ivermectin, Dr. Kory wrote:
The government has lost my trust—and not just with regard to medicine. Climate change, the war in Ukraine, oil shortages, a banking collapse—whatever the new “narrative” is, I’m inclined to suspect it’s usually and mostly false; willfully constructed not for the common good, but for the good of those who control the institutions of society. It’s so bad that I am now even suspicious of the relentless refrain, “Ninety-eight percent of climate change scientists agree that C02 is the root cause of global warming.” Do you know why? Because I heard that same “consensus” about ivermectin, HCQ, and the vaccines. It might be true; it may not be. I may have time to “do my own research” someday; I may not. Regardless, they blew it. I will never again believe a word they say without verifying it myself through exhaustive investigation.
According to SOMO’s research report, “Pharma’s Pandemic Profits,” published on February 27, 2023, Pfizer, BioNTech, Moderna, and Sinovac made an extraordinary $90 billion in profits on their COVID-19 vaccines and medicines in 2021 and 2022. Government National Institutes of Health (NIH) scientists raked in more than $325 million in royalties from Chinese and Russian entities—as well as pharmaceutical companies—for their research on vaccinations. Former National Institutes of Allergy and Infectious Diseases (NIAID) director Dr. Anthony Fauci was among the thousands of government physicians to be paid royalties from pharmaceutical companies between September 2009 and October 2020.
With this much money to be made off COVID-19, it is no wonder the FDA demonized ivermectin (and hydroxychloroquine), common inexpensive medications that possibly could have ended the COVID-19 pandemic before the NIH began demanding that President Trump lock down the U.S. economy. The question now is whether the American public is being set up for another round of COVID-19 scare so big pharma can continue raking in the billions from COVID-19 booster shots that may or may not work.
Most Intensive Ivermectin Use Had 74 Percent Reduction in Excess Deaths in Peru: New Study
Aug 17 2023
According to a new peer-reviewed ecological study, a natural experiment occurred when the government of Peru authorized ivermectin for use during the COVID-19 pandemic resulting in evidence of the drug’s effectiveness and ability to reduce excess deaths.
The paper’s results, published August 8 in Cureus, found a 74 percent reduction in excess deaths in 10 states with the most intensive ivermectin use over a 30-day period following peak deaths during the pandemic. When analyzing data across 25 states in Peru, researchers found these reductions in excess deaths correlated closely to ivermectin use during four months in 2020.
When ivermectin was available without restriction, there was a fourteenfold reduction in nationwide excess deaths. Once access to ivermectin was restricted by the government, a thirteenfold increase in excess deaths was observed in the two months following the limitation of its use. The findings align with summary data from the World Health Organization for the same time period in Peru.
Ivermectin is a widely-known and inexpensive treatment against parasitic diseases. Scientists believe the drug can also bind to the spike protein of the SARS-CoV-2 virus, limiting its morbidity and infectivity.
Peru Promoted Then Restricted Access to Ivermectin
Before Peru implemented COVID-19 vaccine mandates, the country relied on mitigation strategies such as lockdowns and therapeutics to control the SARS-CoV-2 virus that causes COVID-19, as did many other nations.
The Peruvian Ministry of Health, on May 8, 2020, approved ivermectin widely for use prompting 25 states in Peru to implement inpatient and outpatient treatments with ivermectin to different extents and in different time frames. Additionally, through the Mega-Operación Tayta (MOT)—a national program led by the Ministry of Defense—Peru’s government began distributing ivermectin on a wide scale.
Through a partnership with 11 other government agencies, MOT aimed to reach every targeted region with rapid response teams to detect COVID-19 cases, administer ivermectin, and provide food to encourage people to isolate for 15 days. Shortly thereafter, MOT began distributing the therapeutic to everyone identified as high-risk, regardless of whether they tested positive or were symptomatic for COVID-19.
The government of Peru independently tracked daily COVID-19 deaths and all-cause deaths through numerous Peruvian national health databases, allowing researchers to calculate excess deaths. Additionally, they extensively tracked data for deaths and other public health parameters allowing analysis of the potential efficacy of interventions such as ivermectin during the pandemic.
When President Francisco Sagasti took office on Nov. 17, 2020, the government stopped distributing ivermectin and made it available only by prescription. This made the drug significantly more difficult for people to obtain and allowed researchers to see nationwide changes in daily excess all-cause deaths before and after restrictions went into place.
Impact of Ivermectin on Excess Deaths
Excess all-cause deaths were calculated from the total deaths recorded for January through February 2020. During this period, monthly all-cause deaths fluctuated with a mean value of 5.2 percent and a standard deviation of 3.8 percent. By May 2020, total deaths fluctuated by more than double the baseline value calculated in January through February.
An analysis of excess all-cause deaths was performed state-by-state for those aged 60 years and older to establish the date of peak excess deaths during the pandemic’s first wave. Decreases in excess deaths from the peak date of death to 30 and 45 days afterward were tracked. The 25 states were then grouped by the extent of ivermectin distribution: maximal distribution—occurring through operation MOT, medium, and minimal.
Results showed that the 10 MOT states had a sharp decrease in excess deaths after reaching peak values—with a 74 percent drop at 30 days and an 86 percent drop at 45 days after the date of peak deaths. For 14 states that locally administered ivermectin, excess deaths dropped by 53 percent at 30 days and 70 percent at 45 days.
In Lima, where ivermectin treatments were delayed until August—four months after its initial pandemic surge in April—excess deaths only dropped by 25 percent at 30 days and 25 percent at 45 days after peak deaths on May 30.
According to the study, mean reductions in excess deaths 30 days after peak deaths were 74 percent, 53 percent, and 25 percent, respectively, for the maximal, medium, and minimal states that distributed ivermectin. Forty-five days after peak deaths, mean reductions were 86 percent, 70 percent, and 25 percent.
The researchers noted that ivermectin distribution may have yielded such positive numbers due to the drug’s ability to both prevent and treat COVID-19 when distributed to an at-risk population on a greater scale.
Similar Results Observed in Uttar Pradesh, India
Researchers noted similar results with ivermectin distribution in Uttar Pradesh, India, where government teams moved across 97,941 villages as part of a COVID-19 management program to distribute home medication kits that contained ivermectin, doxycycline, zinc, vitamins C and D3, and acetaminophen tablets.
After the mass distribution of ivermectin, the seven-day moving average of COVID-19 deaths in Uttar Pradesh decreased by 97 percent. The cumulative total of COVID-19 deaths per million in population from July 7, 2021, through April 1, 2023, was 4.3 in Uttar Pradesh, compared with 70.4 in all of India and 1,596.3 in the United States, according to the study.
Although Peru had more comprehensive data, the Uttar Pradesh data suggests using ivermectin may prevent and potentially treat COVID-19.
“These encouraging results from IVM [ivermectin] treatments in Peru and similar positive indications from Uttar Pradesh, India, which have populations of 33 million and 229 million, respectively, offer promising models for further mass deployments of IVM, as needs may arise, for both the treatment and prevention of COVID-19,” researchers concluded.
The authors considered factors that could influence their findings, such as the effects of a social isolation mandate imposed in May 2020, the varying genetic makeup of the SARS-CoV-2 virus, differences in seropositivity rates, and population densities across the 25 states. Still, researchers stated the extent and reliability of data showed other factors did not significantly influence study outcomes.
The War on Ivermectin
A lie will circle the world before the truth has a chance to get its' shoes on.

Today lets talk a bit about the history of the use of Ivermectin for treating COVID-19, and in particular the new book which will be out in just a few days from Dr. Pierre Kory and Jenna McCarthy titled “The War on Ivermectin”.
To kick this off, there is a fake/fabricated storyline circulating that the US DoD/DTRA- Chem-Bio defense (DOMANE) program actively suppressed the use of Ivermectin as a COVID-19 treatment option, that I was the leader of the DOMANE program, and that I am personally responsible for the advancement and licensure of Remdesivir and the suppression of Ivermectin as a treatment option. The same self-styled “independent journalist” promoting these obvious falsehoods also asserts that I am responsible for 9-11 and the Anthrax attacks.
The following paragraphs are the first time I have directly addressed aspects of my involvement in drug repurposing for COVID involving Ivermectin.
Historically I primarily have spoken out about the COVID genetic vaccines, because that is what people (and podcasters) wanted to hear from me. But that work is only a small subset of my efforts to provide ways to mitigate the damages caused by SARS-CoV-2, COVID-19 and the COVIDcrisis response since January of 2020. My work in repurposing drugs for early COVID-19 treatment, which consumed all of 2020 and most of 2021, is not something that I have emphasized in my public activities for three general reasons: First, others have spoken at length about their work, so the topic of drug repurposing has been fairly well covered. Second, much of my work was performed as a consultant/subcontractor under various non-disclosure agreements. Nothing nefarious here, just normal business practices for a small consulting shop. Third, despite what some may darkly mutter, my public activities have not been about self-promotion, but rather have been focused on trying to educate and help the general public deal with the upside down clown world of the COVIDcrisis public response that they have been subjected to since January 2020.
I have a general rule of thumb to not talk to the crazies, online or otherwise, and so have not previously felt any particular need to address these various unfounded conspiracy theories promoted by a self-styled “independent journalist” who mostly seems to be obsessed with trying to belittle, gaslight, and denigrate me without bothering to actually do the investigative research which would immediately refute his theories. I have no idea who pays this person to spread his theories and attacks on me and many others.
For the record,
- DOMANE is a DoD/DTRA program. I have never been a DTRA employee. I have never been a member of DTRA (or DOMANE) leadership. All lies. In my role as CEO of my consulting business RWMaloneMD LLC I served as a subcontractor for three DTRA-related contracts. One contract was issued to a small company called Allchem, which at the time was owned by Dr. Jim Talton. That contract was focused on discovering inhibitors of organophosphate toxins (nerve gases and certain pesticides) using high throughput computational and robotic screening methods. The other contract was with MIT Lincoln Lab, where I served as a consultant on that DOMANE contract, which was focused on discovering repurposed drugs for treatment of COVID-19 (including Ivermectin) and advancing sponsored clinical research to test those agents. The third one (also acting as a consultant/subcontractor) was managed by Leidos, and involved development of an advanced patient-centered outcomes research software tool and use in supporting both outpatient (virtual) clinical trials as well as parallel inpatient trials of the repurposed pharmaceutical agents ivermectin, celecoxib, and famotidine. No Remdesivir. Amazingly, the FDA blocked that program (and the DoD) from testing Ivermectin, informing that clinical trials of that agent would not be allowed to proceed until in vitro (in the test tube) studies demonstrated the mechanism of action of Ivermectin as an anti-viral for SARS-CoV-2.
- DOMANE is not the program which advanced and advocated Remdesivir for COVID-19. Another obvious lie. That would be Dr. Anthony Fauci and the NIAID. The historic record is clear on that. DOMANE claims credit for funding the initial development of Remdesivir because it funded the development of this drug as a potential anti-Ebola agent, for which application it failed largely due to toxicity and lack of effectiveness.
- I was an early and continued advocate for use of Ivermectin for treatment of COVID-19. Some, although not this particular “investigative journalist” in question, will remember that I was specifically attacked by “independent journalist” Mr. Alex Berenson for my advocacy of the repurposed agent as a treatment for COVID-19. Reviewing my over 3,400 email correspondences involving Ivermectin since January 01, 2020 (there were many more before that date), I find that the first in this time frame is dated January 10, 2020, and involved internal correspondence with the Alchem team (who were volunteering their time to try to identify repurposed drugs for SARS-CoV-2 treatment). Most are also not aware that further back in time I had been an advocate for the use of Ivermectin as an agent for treating Yellow Fever Virus infection and many other viruses, and even filed a field of use patent (since abandoned) for Ivermectin as an antiviral.
- Searching my email accounts for the key words “Ivermectin” and “Kory” (as in Pierre) reveals 936 email correspondences, the first being on 11/19/2020 (almost 200 days prior to the Bret Weinstein/Pierre Kory DarkHorse Podcast. This first notification of the potential efficacy of Ivermectin was part of a summary provided by senior (since retired) DTRA/DOMANE scientist Dr. Howard Haimes. On December 08, 2020, I wrote to the project officer for the DTRA/DOMANE contractor Leidos concerning the following article posted on Trial Site News, and advocating for clinical testing of Ivermectin within the funded program:
Prominent Physician/Researchers to Present Case for Ivermectin to U.S. Senate Committee on Homeland Security & Governmental Affairs
The U.S. Senate Committee on Homeland Security & Governmental Affairs will hold a full committee hearing on December 8, 2020, at 10:00 AM at the Senate Dirksen Building and via video conference. Titled “Early Outpatient Treatment: An Essential Part of a COVID-19 Solution, Part II,” invited witnesses to include Jane M. Orient, MD, Executive Director Association of American Physicians and Surgeons, Pierre Kory, MD, Associate Professor of Medicine, St. Luke’s Aurora Medical Center, Jean-Jacques Rajter, MD, Pulmonologist, Broward Health Medical Center and ICON study co-author and Ramin Oskoui, MD, Vice President of Medical Staff, Sibley Memorial Hospital and Chief Executive Officer of Foxhall Cardiology. Prominent among discussion topics will be the use of ivermectin as a treatment for early-stage, mild to moderate COVID-19 cases. To date, although well over $12 billion U.S. dollars have been spent by the taxpayers, there has been no breakthrough for early-stage treatment, an incredibly important period to get COVID-19 under control. There is evidence that some generic-based treatments can help accomplish this objective.
In the same email, I further advocated for clinical trial testing of Ivermectin by including a link to this website:
COVID-19 treatment studies for Ivermectin
On December 05, 2020, I reached out to Pierre’s co-author on an informal review of Ivermectin as a COVID-19 treatment (which had been published informally on the internet), which lead to my being introduced to Pierre, launching what I hope will be a lifelong friendship.
Dear Dr Lieberman,
Alexis - Please consider preparing and submitting a report summarizing experiences treating COVID-19 with Ivermectin! We have set up this special topic of Frontiers in Immunology specifically so that there will be a forum for physicians and scientists such as yourself to report observations that may not yet meet the criteria for publication in high profile journals, but which are not otherwise being reported and published. This journal is "open source", and so does charge for managing and formatting each publication. Best wishes Robert Malone, MD, MS
Frontiers in Pharmacology has launched a new Research Topic, Treating COVID-19 With Currently Available Drugs. As a leading expert in your field, we would like you to participate by submitting your research.
Pierre wrote back on December 11, 2020:
Alexis, Robert,
Thank you for making our acquaintance and I so appreciate your mention of the short period to publication because:
We know many many lives are at stake with every day that this manuscript takes through peer review. I cannot stress this enough
I am just now getting offers from other journals also emphasizing speed. I am much more attracted to quality and speed right now than just impact factor etc (this is also a first for me in publishing manuscripts, i.e. journals reaching out to me
Anyway, Robert, I thank you for your interest, it is very encouraging – do you know what kind of time-line to on-line publication we can expect if it passes peer review and/or requires only minor revisions. If anything more gets required, we understand it would take much longer. Anyway, thanks for your interest and please advise – thanks, Pierre
Pierre Kory, MD, MPA
President, Front-Line Covid-19 Critical Care Alliance
Associate Professor of Medicine
Advocate Aurora Critical Care Service
St. Luke’s Aurora Medical Center, Milwaukee, WI
Front Line COVID-19 Critical Care Alliance
Prophylaxis & Treatment Protocols for Covid-19
www.covid19criticalcare.com
www.flccc.net
Thus launched at initiative which unfortunately ended poorly. Pierre submitted his manuscript to Frontiers and I was assigned as editor for the submission. I selected four highly qualified reviewers - 1) a senior pharmaceutical scientist, 2) the most senior FDA clinical reviewer, 3) another senior FDA pharmaceutical scientist from the office of the Chief Scientist, and 4) a front line ICU physician practicing at a major academic medical center in NYC/Brooklyn. These four put the manuscript through extensive review and revisions. It was accepted for publication. Pierre and the FLCCC paid the required publication fee. As was the usual practice for Frontiers in Pharmacology, the abstract was published as a pre-print/teaser. It accrued a record number of views in just a few short days. And then all hell broke loose.
The editor in chief of Frontiers forced the paper to be withdrawn. This set off a cascade which eventually lead to resignation of the editors (including myself) who had created this special edition of Frontiers in Pharmacology specifically to enable publication of COVID-19 repurposed drug research, and closing down of that special volume without publication. At the time, the Editor in Chief was warned that if he took these actions, he would be responsible for large numbers of avoidable deaths. Time has validated that assertion, along with so many others which were made along the way but attacked at the time.
The resulting mess (and Frontiers’ denials of culpability) were then covered in two articles by a UK publication named “The Scientist”:
Frontiers Removes Controversial Ivermectin Paper Pre-Publication
A review article containing contested claims about the tropical medicine drug as a COVID-19 treatment was listed as “provisionally accepted” on the journal’s website before being removed this week.
Frontiers Pulls Special COVID-19 Issue After Content Dispute
The issue’s guest editors resign after falling out with the publisher over the management of papers, including a rejected manuscript on ivermectin, that were submitted for a special issue on drug repurposing for COVID-19.
So, I ask you. Based on the evidence above, did I serve as the leader of DOMANE, act to promote Remdesivir and block Ivermectin? These are lies which are being promoted for some undisclosed ulterior motive by someone who self-identifies as an “investigative journalist” and has posted literally thousands of on-line attacks on my character and integrity. As are the assertions that I am somehow responsible for 9-11 and the Anthrax attacks (at which time I was actually living in Rockville MD working on developing a Breast Cancer research facility and tissue bank in Windber, PA under a John Murtha porkbarrel project called the Windber Research Institute, while also starting a US-based company called Inovio).
The record clearly shows that I was an early and strong advocate for use of Ivermectin (and celecoxib, and famotidine) as repurposed drug agents for treating COVID-19, and a strong advocate for the work of Dr. Pierre Kory and his colleagues at the FLCCC.
The good news to come out of this horrid chapter in the COVIDcrisis story was that through all of this drama and trauma, and subsequently in so much other travel (thousands of emails!), meetings and discussions (including both “DEFEAT THE MANDATES” rallies, I have been able to develop what I hope will be a livelong friendship with Dr. Pierre Kory and his close colleague Dr. Paul Marik.
Dr. Pierre Kory is the kind of guy people love to love. A native New Yorker with a huge heart and a knack for numbers, Kory is equal parts affable and academic, quick to crack a joke or rattle off complex medical statistics from memory. He’s been on the Covid front lines from the beginning, searching for answers, testifying before the senate, and advocating for both patient and physician rights—a journey he eloquently and assiduously documents in his forthcoming book, The War on Ivermectin (Skyhorse, June 2023). Kory has been called everything from a fringe doctor to a medical misinformationist—two terms that in today’s upside-down world translate into “someone you definitely want to listen to.” It’s my pleasure to share the first chapter of his book, written with author Jenna McCarthy and featuring a foreword by Del Bigtree. Kory’s is a powerful, highly-anticipated story filled with facts, humor and truth that will edify and enlighten readers around the world.
The War on Ivermectin, Chapter One: Before the Beginning
Here’s to the crazy ones. The misfits. The rebels. The troublemakers. The round pegs in the square holes. The ones who see things differently. They’re not fond of rules. And they have no respect for the status quo. You can quote them, disagree with them, glorify or vilify them. About the only thing you can’t do is ignore them. Because they change things. They push the human race forward. And while some may see them as the crazy ones, we see genius. Because the people who are crazy enough to think they can change the world are the ones who do.
—Steve Jobs
I do quite a bit of public speaking these days, and part of my schtick has become somewhat of an “ode to the old Pierre.” When I say old, of course, I mean pre-Covid.
Old Pierre believed that the elite, esteemed medical journals represented the best of scientific thought and study. The Lancet or the New England Journal of Medicine said so? It was settled then. Old Pierre religiously read the New York Times from cover to cover, because it was the paper of record; the arbiter of truth. If you wanted to know what was really going on, you read the Times. Period. He voted for Biden (although in his defense, he wasn’t exactly a fan and never put a BIDEN-HARRIS ring around any of his social media profile photos), trusted the government (I know!), and actually believed that public health agencies were committed to safeguarding and improving . . . wait for it . . . public health. He knew—knew, I tell you!—that vitamins were a scam and that hospitals were life-saving centers of care, compassion, and excellence. Old Pierre dutifully lined up for his own annual flu shot and followed the childhood immunization schedule to the letter with his three daughters.
He was a clueless sonofabitch.
Nobody, least of all me, could have predicted the insane series of events, discoveries, and decisions that would transform him (me) into the wildly different doctor—and man—that I am today.
But here we are.
So this is my story. What started as a daily brain dump, a place to record the happenings and heartbreaks occurring at work and at home, slowly morphed into this crazy peek into a decidedly broken medical system. I set out to understand and expose what was happening with repurposed drugs, ivermectin specifically. By October of 2020, we had identified an inexpensive, safe, widely available medication that was showing tremendous potential not just as a treatment for Covid but also as a preventative. As the weeks and months wore on, the data supporting its safety and efficacy were astounding. And yet the backlash against it was swift and furious. Positive studies were overturned and retracted. Negative studies appeared out of thin air. Around the world it was quietly being used to tremendous, almost impossible success, and yet doctors were punished for prescribing it, pharmacies refused to fill valid prescriptions for it, and the media would only touch it to call it “the horse dewormer.” To a physician fighting on the front lines of this battle, this systematic smear campaign was unfathomable.
I soon discovered that the corruption and deceit were hardly limited to the pharmaceutical space. The entire medical industrial complex—including our governmental and international regulatory agencies, Big Pharma, public and private health care systems and hospital networks, medical schools and their journals, and at least one centi-billionaire “philanthropath”—had been collectively captured. According to Wikipedia (which I don’t often use as a reference source, incidentally, but their explanation was most succinct), “When regulatory capture occurs, a special interest is prioritized over the general interests of the public, leading to a net loss for society.”1
You can say that again.
At the risk of sounding arrogant or self-congratulatory, when it came to Covid, I got a lot of things right from the beginning. So often and so overwhelmingly, in fact, that I was dubbed “Lucky Pierre,” first by the editor of the New England Journal of Medicine in a magazine interview, and then by my colleagues and friends. I want to acknowledge here, up front, that I ascribe much of that consistent, almost implausible “rightness” to this: practically from day one, I was part of a group of highly credible, extensively experienced professors, scientists, and clinicians who were deeply studied on nearly every aspect of medicine even remotely related to Covid. We shared a spirit and a purpose well before we had a name (the Front Line Covid Critical Care Alliance, or FLCCC), a website, or a nonprofit designation.
The whole is always greater than the sum of its parts, and that is exponentially true with the FLCCC. After all, we’re the misfits, the troublemakers, the round pegs in the square holes. We’re the ones standing up to the system; the child watching the bare-assed Emperor parade down the street who just can’t hold his tongue.
“But he hasn’t got anything on,” we’ve been shouting. At first, people pointed and laughed at us and called us names, but we didn’t care. That fat bastard was naked, and nothing could make us see or think otherwise! And do you know what? People are starting to catch on. More and more, some might say in droves, they’re seeing what we see and have seen for a few years now.
That is the power and spirit of the collaboration and camaraderie behind the FLCCC. From the beginning, we were bound by mutual passion and respect, and committed to uncovering and speaking the truth—no matter how difficult or isolating that proved to be.
So yeah, we’ve gotten a lot right. It turns out, that’s actually not so hard to do when you’re surrounded by greatness and your hearts are in the right place.
Excerpted from The War on Ivermectin by Dr. Pierre Kory with Jenna McCarthy
Is Quercetin a Safer Alternative to Hydroxychloroquine?
Feb 10 2023
(photo_gonzo/Shutterstock)
Evidence suggests hydroxychloroquine works for COVID-19 because it acts as a zinc ionophore, meaning it shuttles zinc into your cells. Canadian and Chinese researchers are collaborating on a study to assess the effectiveness of this alternative powerful immune booster and broad-spectrum antiviral.
STORY AT-A-GLANCE
- A Chinese trial comparing clinical outcomes of COVID-19 patients treated with the antimalarial drug hydroxychloroquine and those receiving standard of care alone reports “disappointing” results.
- The hydroxychloroquine group only had a 28-day negative conversion rate of 85.4 percent compared to the control group’s rate of 81.3 percent. No difference in the alleviation of symptoms was observed between the two groups.
- The study did not, however, use supplemental zinc, which helps prevent viral replication. Evidence suggests hydroxychloroquine works for COVID-19 because it acts as a zinc ionophore, meaning it shuttles zinc inside your cells.
- A Brazilian chloroquine trial stopped the high-dose arm of the study early due to patients developing ventricular tachycardia, a dangerous heart rhythm problem. Chloroquine is known to be more toxic than hydroxychloroquine.
- Quercetin is a naturally occurring zinc ionophore. Taken with zinc, it may be helpful to prevent and potentially treat COVID-19. Research is currently underway to assess quercetin’s effectiveness against COVID-19.
The debate about whether the antimalarial drug hydroxychloroquine is an effective treatment for COVID-19 continues, as a Chinese trial (1)(2)(3) comparing clinical outcomes of those treated with the drug and those receiving standard of care alone reports “disappointing” results.
Hydroxychloroquine Trial Reports Disappointing Results
Seventy-five COVID-19 patients at 16 Chinese treatment centers received 1,200 milligrams of hydroxychloroquine (HCQ) in addition to standard of care for the first three days of treatment, followed by a maintenance dose of 800 mg per day for two weeks in mild to moderate cases and three weeks for severe cases. Another 75 patients received standard of care only.
The primary endpoint was a 28-day negative conversion rate of SARS-CoV-2 (viral load reduction). Secondary endpoints included an improvement rate of clinical symptoms and the normalization of C-reactive protein and blood lymphocyte count within 28 days.
According to the authors, the hydroxychloroquine group only had a 28-day negative conversion rate of 85.4 percent compared to the control group’s rate of 81.3 percent. No difference in the alleviation of symptoms was observed between the two groups.
Adverse events were also higher in the hydroxychloroquine group (30 percent) compared to controls (8.8 percent). You can find a listing of the adverse events in Table 2 of the study. (4)
The most common adverse event, at 10 percent, was diarrhea. That said, the authors point out that: (5)
“A significant efficacy of HCQ [hydroxychloroquine] on alleviating symptoms was observed when the confounding effects of anti-viral agents were removed in the posthoc analysis (Hazard ratio, 8.83, 95 percent CI, 1.09 to 71.3).
“This was further supported by a significantly greater reduction of CRP [c-reactive protein] (6.986 in SOC [standard of care] plus HCQ versus 2.723 in SOC, milligram/liter, P=0.045) conferred by the addition of HCQ, which also led to more rapid recovery of lymphopenia, albeit no statistical significance.
“Conclusions: The administration of HCQ did not result in a higher negative conversion rate but more alleviation of clinical symptoms than SOC alone in patients hospitalized with COVID-19 without receiving antiviral treatment, possibly through anti-inflammatory effects. Adverse events were significantly increased in HCQ recipients but no apparent increase of serious adverse events.”
Limitations of This Study
A few things are worth noting about this study. Aside from its small size, the patients received a far higher dose of hydroxychloroquine than typically used in the U.S.—1,200 milligrams for the first three days, followed by 800 mg per day for two to three weeks, compared to the U.S. Food and Drug Administration’s suggested dosage of 800 mg on day one, followed by 400 mg per day for four to seven days, depending on severity. (6)
Secondly, most patients had mild disease with little hypoxemia, and thirdly, treatment was administered quite late, on average 16 to 17 days after the onset of disease. Commenting on the findings, Josh Farkas, associate professor of pulmonary and critical care medicine at the University of Vermont wrote:
“Much of the pathogenesis of critical illness seems to result from dysregulated inflammation, rather than direct viral cytopathic effect. This raises a question of whether any antiviral treatment will be beneficial for late-presenting patients with severe illness.
“Of course, it is possible that earlier use of hydroxychloroquine could be beneficial (e.g., perhaps at the first signs of illness on an out-patient basis). This is under investigation and additional data is likely to be forthcoming soon. Even if this does work in the outpatient clinic, it would probably have little impact on the management of these patients within the intensive care unit.”
Editor’s note: This blog was deleted and wiped clean from the internet later. I am leaving it here to illustrate how something controversial can quickly disappear, even when well-documented and sourced at the time it’s used.
This Study Failed to Use Zinc
Perhaps most important, however, is the absence of zinc, which Farkas does not mention. We now know that chloroquine and hydroxychloroquine act as zinc ionophores, (7)(8) meaning they shuttle zinc into your cells, and zinc appears to be a “magic ingredient” required to prevent viral infection. (9)
If given early, zinc along with a zinc ionophore should, at least theoretically, help lower the viral load and prevent the immune system from becoming overloaded. Without zinc, hydroxychloroquine may be more or less useless.
So, in my view, I doubt this study is worth placing too much stock in, seeing how it did not administer supplemental zinc. As noted in the preprint paper, “Does Zinc Supplementation Enhance the Clinical Efficacy of Chloroquine/Hydroxychloroquine to Win Today’s Battle Against COVID-19?” published April 8, 2020: (10)
“Besides direct antiviral effects, CQ/HCQ [chloroquine and hydroxychloroquine] specifically target extracellular zinc to intracellular lysosomes where it interferes with RNA-dependent RNA polymerase activity and coronavirus replication.
“As zinc deficiency frequently occurs in elderly patients and in those with cardiovascular disease, chronic pulmonary disease, or diabetes, we hypothesize that CQ/HCQ plus zinc supplementation may be more effective in reducing COVID-19 morbidity and mortality than CQ or HCQ in monotherapy. Therefore, CQ/HCQ in combination with zinc should be considered as an additional study arm for COVID-19 clinical trials.”
Chloroquine Trial Stopped Due to Side Effects
In related news, a Brazilian chloroquine trial (11) (12) stopped the high-dose arm of the study early due to patients developing ventricular tachycardia, a dangerous heart rhythm problem. As reported by Live Science: (13)
“The Brazilian researchers planned to enroll 440 people in their study to test whether chloroquine is a safe and effective treatment for COVID-19. Participants took either a ‘high dose’ of the drug (600 milligrams twice daily for 10 days) or a ‘low dose’ (450 mg for five days, with a double dose only on the first day) …
“However, after enrolling just 81 patients, the researchers saw some concerning signs. Within a few days of starting the treatment, more patients in the high-dose group experienced heart rhythm problems than did those in the low-dose group. And two patients in the high dose group developed a fast, abnormal heart rate known as ventricular tachycardia before they died.”
As explained in my previous article, “Antimalarial Medications: A COVID-19 Treatment Option?” chloroquine and hydroxychloroquine have been shown to be effective in the lab against the SARS coronavirus that appeared in 2003. (14)(15)(16) Laboratory testing also suggests chloroquine is effective in cell cultures against COVID-19 when combined with an antiviral drug, remdesivir. (17)
However, chloroquine (Aralen) appears to be a more hazardous choice than hydroxychloroquine (Plaquenil), which is a derivative of chloroquine. (18) Both use the same pathway, but hydroxychloroquine is thought to be about 40 percent less toxic (19) and, overall, has a safer side effect profile. (20)(21)
Quercetin is found in berries, citrus fruits, grapes, and more. (pilipphoto/Shutterstock)
Quercetin–A Safer Alternative to Hydroxychloroquine?
Considering the risks of chloroquine and hydroxychloroquine, and the evidence suggesting the reason these drugs work for COVID-19 is because they act as zinc ionophores, it’s worth questioning whether other more natural zinc ionophores can be used.
One prime example would be quercetin, which is a naturally occurring zinc ionophore. (22) As reported by the Green Stars Project, (23) “Researchers from Oak Ridge National Lab used the world’s most powerful supercomputer, SUMMIT, to look for small molecules that might inhibit the COVID-19 spike protein from interacting with human cells and, interestingly, quercetin is fifth on that list.” (24)
Quercetin is one of only three natural products found to inhibit the SARS-CoV-2 spike protein. The only natural product found to be slightly more effective is luteolin, a polyphenol found in radicchio, green peppers, serrano and green hot chili peppers, chicory, celery, and many other foods. (25)
Quercetin is another flavonols compound found in a variety of foods, including apples, Brassica vegetables, capers, onions, tea, and tomatoes, just to name a few. It’s also contained in medicinal products such as ginkgo biloba, St. John’s Wort (Hypericum perforatum), and elderberry (Sambucus canadensis).
Research has already demonstrated that quercetin is a powerful immune booster and broad-spectrum antiviral. As noted in a 2016 study (26) in the journal Nutrients, quercetin’s mechanisms of action include the inhibition of lipopolysaccharide (LPS)-induced tumor necrosis factor α (TNF-α) production in macrophages.
TNF-α is a cytokine involved in systemic inflammation, secreted by activated macrophages, a type of immune cell that digests foreign substances, microbes, and other harmful or damaged components. Quercetin also inhibits the release of pro-inflammatory cytokines and histamine by modulating calcium influx into the cell. (27)
According to this paper, quercetin also stabilizes mast cells and has “a direct regulatory effect on basic functional properties of immune cells,” which allows it to inhibit “a huge panoply of molecular targets in the micromolar concentration range, either by down-regulating or suppressing many inflammatory pathways and functions.” (28)
Another 2016 study (29) concluded it helps modulate the NLRP3 inflammasome, an immune system component involved in the uncontrolled release of pro-inflammatory cytokines that occurs during a cytokine storm.
In vitro studies (30)(31)(32) have shown quercetin exerts antiviral activity against SARS-CoV, and preliminary findings (33) suggest quercetin can inhibit the SARS-CoV-2 main protease as well. You can get even more details about the anti-inflammatory and antiviral powers of quercetin in “Quercetin Lowers Your Risk for Viral Illnesses.”
Quercetin Being Studied for Its Use Against COVID-19
The good news is researchers are in fact planning to study the use of quercetin against COVID-19. (34) As reported by Maclean’s, (35) Canadian researchers Michel Chrétien and Majambu Mbikay began investigating quercetin in the aftermath of the SARS epidemic that broke out across 26 countries in 2003.
They discovered a derivative of quercetin provided broad-spectrum protection against a wide range of viruses, including SARS. (36)(37) The Ebola outbreak in 2014 offered another chance to investigate quercetin’s antiviral powers and, here too, they found it effectively prevented infection in mice, “even when administered only minutes before infection.”
So, when the COVID-19 outbreak was announced in Wuhan City, China, in late December 2019, Chrétien contacted colleagues in China with an offer to help. In February 2020, Chrétien and his team received an official invitation to begin clinical trials. According to Maclean’s: (38)
“The Canadian and Chinese scientists would collaborate on the trials, which would include about 1,000 test patients. Chrétien and Mbikay plan to join colleagues from the non-profit International Consortium of Antivirals—which Chrétien co-founded with Jeremy Carver in 2004 as a response to the SARS epidemic—in manning a 24/7 communications center as soon as clinical trials go ahead.
“The U.S.-based Food and Drug Administration has already approved quercetin as safe for human consumption, which means the researchers can skip testing on animals. If the treatment works, it’ll be readily available … Chrétien’s team says their treatment would cost only $2 a day.”
Dosage Recommendations for Quercetin and Zinc
While the COVID-19 pandemic is in full swing—and for any future influenza season—supplementing with quercetin and zinc may be a good idea for many, in order to boost your immune system’s innate ability to ward off infectious illness. As for dosage, here are some basic recommendations:
- Quercetin: According to research from Appalachian State University in North Carolina, taking 500 mg to 1,000 mg of quercetin per day for 12 weeks results in “large but highly variable increases in plasma quercetin … unrelated to demographic or lifestyle factors.” (39)
- Zinc (and copper): When it comes to zinc, remember that more is not necessarily better. In fact, it can backfire. When taking zinc, you also need to be mindful of maintaining a healthy zinc-to-copper ratio. As noted by Chris Masterjohn, who has a doctorate in nutritional sciences,(40) in an article (41) and series of Twitter posts: (42)
“In one study, 300mg/day of zinc as two divided doses of 150 mg zinc sulfate decreased important markers of immune function, such as the ability of immune cells known as polymorphonuclear leukocytes to migrate toward and consume bacteria.
“The most concerning effect in the context of COVID-19 is that it lowered the lymphocyte stimulation index threefold. This is a measure of the ability of T cells to increase their numbers in response to a perceived threat. The reason this is so concerning in the context of COVID-19 is that poor outcomes are associated with low lymphocytes …
“The negative effect on lymphocyte proliferation found with 300 mg/day and the apparent safety in this regard of 150 mg/d suggests that the potential for hurting the immune system may begin somewhere between 150-300 mg/d …
“It is quite possible that the harmful effect of 300 mg/d zinc on the lymphocyte stimulation index is mediated mostly or completely by induction of copper deficiency …
“The negative effect of zinc on copper status has been shown with as little as 60 mg/d zinc. This intake lowers the activity of superoxide dismutase, an enzyme important to antioxidant defense and immune function that depends both on zinc and copper …
“A study done with relatively low intakes of zinc suggested that acceptable ratios of zinc to copper range from 2:1 to 15:1 in favor of zinc. Copper appears safe to consume up to a maximum of 10 mg/d.
“Notably, the maximum amount of zinc one could consume while staying in the acceptable range of zinc-to-copper ratios and also staying within the upper limit for copper is 150 mg/d.”
How Much Zinc Do You Need?
Masterjohn goes into even greater detail in his zinc article, discussing maximum absorption rates and much more. (43) In summary, he recommends taking 7 mg to 15 mg of zinc four times a day, ideally on an empty stomach, or with a phytate-free food.
The recommended dietary allowance in the U.S. is 11 mg for adult men and 8 mg for adult women, with slightly higher doses recommended for pregnant and breastfeeding women, (44) so we’re not talking about taking significantly higher dosages.
Additionally, you can take one zinc acetate lozenge per day, which will provide you with an additional 18 mg of zinc. If you’re exposed to the virus, take one additional lozenge after the exposure.
Masterjohn stresses that you’ll want to keep your total zinc intake below 150 mg per day to avoid negative effects on your immune system. He also recommends getting at least 1 mg of copper from food and supplements for every 15 mg of zinc you take.
Keep in mind that there are many food sources of zinc, so a supplement may not be necessary. I eat about three-fourths of a pound of ground bison or lamb a day, which has 20 mg of zinc. I personally don’t take any zinc supplement other than what I get from my food, which is likely in an optimal form to maximize absorption.
Originally published April 27, 2020, on Mercola.com
◇ References:
(1) Medrxiv.org April 14, 2020 DOI: 10.1101/2020.04.10.20060558 [Preprint]
(2) Medrxiv.org April 14, 2020 DOI: 10.1101/2020.04.10.20060558 [Preprint] (PDF full study)
(4) Medrxiv.org April 14, 2020 DOI: 10.1101/2020.04.10.20060558 [Preprint] (PDF) Table 2, Page 37
(5) Medrxiv.org April 14, 2020 DOI: 10.1101/2020.04.10.20060558 [Preprint]
(6) FDA.gov Fact Sheet, EUA of Hydroxychloroquine (PDF)
(7) PLOS ONE 2014; 9(10): e109180
(8) Preprints April 6, 2020 DOI: 10.20944/preprints202004.0124.v1
(9) Preprints April 6, 2020 DOI: 10.20944/preprints202004.0124.v1
(10) Preprints April 6, 2020 DOI: 10.20944/preprints202004.0124.v1
(11) Medrxiv.org April 11, 2020 DOI: 10.1101/2020.04.07.20056424
(12) Medrxiv.org April 11, 2020 DOI: 10.1101/2020.04.07.20056424 (PDF full study)
(13) Live Science April 13, 2020
(14) Antiviral Research, 2020;177:104762 Highlight bullest
(15) Clinical Infectious Disease, 2020; 10.1093/cid/ciaa237 Abstract
(16) Virology Journal, 2005;2(69) Abstract/Conclusion
(17) Cell Research, 2020;30:269 Abstract
(18) Nature March 18, 2020; 6 Article number 16, Correspondence
(19) Nature March 18, 2020; 6 Article number 16, Correspondence
(20) Clinical Infectious Diseases, 2020; doi.org/10.1093/cid/ciaa237 Abstract
(21) Medicinenet.com Chloroquine vs Hydroxychloroquine
(22) Journal of Agricultural and Food Chemistry 2014, 62, 32, 8085-8093
(23) Greenstarsproject.org March 27, 2020
(24) ChemRxiv.org March 11, 2020 (PDF full study), Table 3
(25) Myintakepro.com Luteolin Rich Foods
(26) Nutrients 2016 Marck; 8(3): 167, 5.1.2 Mechanism of Action
(27) Nutrients 2016 March; 8(3): 167, Table 1: Mast cell
(28) Nutrients 2016 March; 8(3): 167, 5.1.2 Mechanism of Action
(29) Mediators of Inflammation 2016; 2016, Article ID 5460302
(30) Journal of Virology Oct. 2004: 11334-11339 (PDF)
(31) Biotechnology Letters Feb. 15, 2012; 34: 831-838
(32) Bioorg Med Chem 2010 Nov 15;18(22):7940-7
(33) Preprints.org March 12, 2020
(34) CBC Feb. 28, 2020
(36) Bioorg Med Chem. 2006 Dec 15;14(24):8295-306
(37) Journal of Virology Sep 2004, 78 (20) 11334-11339, Antiviral activity of an analog of luteolin
(41) Chrismasterjohnphd.com Best Dose of Zinc for COVID-19 Prevention
(42) Twitter, Chris Masterjohn April 10, 2020
(43) Chrismasterjohnphd.com Best Dose of Zinc for COVID-19 Prevention
(44) NIH Zinc Fact Sheet
Ivermectin Is Safe and Effective: The Evidence
Dec 25 2022
Decades of use with nearly four billion doses to humans preceded recent use with COVID patients. From the chapter ‘Ivermectin sends COVID to lockdown,’ in my book The Defeat Of COVID.
Ivermectin is on the World Health Organization (WHO) List of Essential Medicines and is approved by the US Food and Drug Administration (FDA). This well-tolerated but potent anti-parasitic medicine has been prescribed billions of times in its 36-year history against a wide range of parasites. It is a drug in the avermectin family, so named because those compounds are produced by the soil organism Streptomyces avermitilis. It has also been studied and used against a wide range of viruses especially over the last decade, and there is evidence of potent antiviral effects against Influenza A and over a dozen other viruses tested. [309]
In a meta-analysis of 63 studies of ivermectin versus COVID-19 in humans, 100% of these have shown positive results. Studies were from all continents except Antarctica. Considered individually, 29 of those studies were found to be statistically significant regarding use of ivermectin alone. Over the 63 studies in meta-analysis, pooled effects showed 69% improvement in early treatment, and prophylactic use showed 86% improvement. Of those studies in the meta-analysis that were peer-reviewed, overall improvement in early treatment was found to be 70% (64% in randomized controlled trials), and 86% of those in which ivermectin was used prophylactically showed improvement (84% in randomized controlled trials).
Mortality from COVID-19 over all time periods of delay in treatment was 76% improved over controls (69% in randomized controlled trials), whereas mortality was improved 84% in early treatment of COVID-19 (82% in randomized controlled trials). Forty studies were excluded from the meta-analysis for complicating factors or insufficient detail reported, and these also showed 100% positive results.
It is estimated that the likelihood of an ineffective treatment showing such positive results as the above results in the 63 studies in the meta-analysis to date is exceedingly small. That probability is estimated to be one in one trillion. [310] The overall results of the meta-analysis were not only found to be “overwhelmingly positive,” but also “very consistent, and very insensitive to potential selection criteria, effect extraction rules, and/or bias evaluation.” The data in the meta-analysis are as of date of this article, and are continually updated as new studies are reported.
The first clinical trial of ivermectin in COVID-19 patients was an observational study in four Florida hospitals from March to May 2020. Even in patients with severe pulmonary involvement, mortality was 38.8% in the treatment group vs 80.7% in controls, and this group showed the strongest mortality difference from controls, which raised the possibility of ivermectin also being available as a salvage or rescue treatment. [311]
In a randomized controlled trial, patients given ivermectin were 8 times more likely to be medically released than those in the placebo group. This was even though the average age and number of comorbidities were later found to be somewhat higher in the experimental group than in the control group. [312]
The African continent has had remarkably low incidence of COVID-19, particularly equatorial African countries. It may be helpful to look at African countries where ivermectin has been used commonly for decades against the onchocerciasis that it has been prescribed for, to observe population-wide effects. In this population comparison, risk of COVID-19 death was found to be 88.2% lower and morbidity 85.7% lower in 31 countries where onchocerciasis is endemic and ivermectin is commonly used than in 22 countries where neither is the case, even though the latter group of countries has a higher life expectancy, 66 years vs 61 years. [313]
Ivermectin, for all its power against viruses, is among the safest of medicines that are in long-term and widespread use. [314] There are no known serious drug-related adverse events. [315] Again, it is commonly taken by the populations of 31 African countries for effect against endemic parasites. Dosing has been given as a single annual dose of 150 mcg/kg against filariasis. There have been very few serious adverse events reported over more than 30 years of use. 37 of approximately 14,000 patients treated in Ghana had symptomatic posture hypotension, associated with fainting or sweating or tachycardia. These were treated with corticosteroids. [316] This Lancet study determined its safety in pregnant women, and the risk of fetal damage was not greater than in control women’s fetuses. [317]
However, despite this safety data going back 3 decades, the US FDA has alleged, “Any use of ivermectin for the prevention or treatment of COVID-19 should be avoided as its benefits and safety for these purposes have not been established.” The FDA offered no supporting evidence for their claim. [318] One concerning risk is that ivermectin is sold over the counter for veterinary use, and if people feel desperate to use it to ward off COVID-19, they might break off too large a piece from a large horse pill. For this reason, it is much better to consult a healthcare provider for ivermectin use and dosing. To further enhance safety, liposomal ivermectin carriers have been developed. When these were used against Dengue fever, cytotoxicity was reduced up to 5 times, absorption was faster and in vivo efficacy was improved. [319]
Despite the spectacular worldwide effect profile, of excellent effect against COVID-19, with 0.26% observed minor side effects, and its use across several continents, ivermectin is widely shunned and ignored in western Europe and in the US. Here is a brief synopsis of how that came to be.
Ivermectin was invented in Japan in 1975 as an anti-parasitic drug by Satoshi Omura, a Kitasato University professor emeritus, which earned Dr. Omura the Nobel Prize in Biochemistry. Ivermectin turned out to be quite effective against a broad spectrum of parasites. The drug was so effective in eliminating a range of parasitic infections, and at very low cost, about $0.10 US, that 3.7 billion doses have been delivered to much of the world’s population since its invention. [320]
A cell culture study in April 2020 showed a 5000 times reduction in SARS-CoV-2 from one dose over 48 hours, compared to control samples. [321] Several Latin American countries, Egypt and India soon began to use it for COVID-19, and then South Africa and several European countries as well. However, resistance remained strong in the US and western Europe, following the vocal disapproval of The World Health Organization (WHO), The US National Institutes of Health (NIH), the US Food and Drug Administration (FDA) and the European Medicine Agency (EMA). These agencies all expressed disapproval of ivermectin for use with COVID-19 patients. Even after more than 20 randomized controlled clinical trials showed promising effect without adverse reactions, many western countries have still not adopted its use.
Caly, Druce, et al illustrate the IMP inhibition as follows:

Figure © L Caly, J Druce, et al., Endnote 321
Social media companies censored ivermectin research. Even when the WHO commissioned and reported a meta-analysis of ivermectin, it was censored by YouTube. Only negative commentaries were permitted in western media. [322]
How does ivermectin send SARS-CoV-2 to lockdown? There are a number of mechanisms by which components of SARS-CoV-2 need to stay mobile and active in order to replicate, and thus to spread throughout the human body. It turns out that ivermectin binds several of these, which inactivates the virus. Let’s look at exactly what happens to bind or to lock down SARS-CoV-2.
RNA-dependent RNA-polymerase (RdRp) is one of the main enzymes used by SARS-CoV-2 to achieve RNA replication. It is required for viral genome replication, and therefore it is helpful if a nutrient or drug can act on it as an obstacle in some way. 173 drugs were tested in this study for their ability to bind RdRp (making it unavailable or inactive), including two examined in this book, hydroxychloroquine and vitamin C, although vitamin C was also found to have relatively high binding energy for RdRp in this study. Of all the drugs tested, ivermectin was found to bind RdRp with higher binding any energy than any other drug. [323]
One strategy against SARS-CoV-2, as well as other endemic and pandemic RNA viruses, has been to interfere with transport of viruses into a host cell’s nucleus. Ivermectin has been shown to accomplish this by binding, destabilizing and inhibiting the protein IMP alpha/beta1. When this protein is inhibited, viruses are unable to enter a cell’s nucleus, and therefore unable to replicate. Decreased infection results. IMP alpha/beta 1 has been inhibited in SARS-CoV-2 entry into nuclei by ivermectin. [324] Previously, it has been observed that ivermectin inhibited that same protein from entry of other RNA viruses, giving it a broad-spectrum antiviral effect. [325] [326] [327]
It turns out that ivermectin not only binds tightly to RdRp on SARSCoV-2, and IMP alpha/beta1; it also strongly binds the spike protein on SARS-CoV-2. This particular spike protein is trimeric, meaning it has 3 subunits which vary in amino acid sequences or other ways. It was observed that ivermectin binds all three of the SARS-CoV-2 subunits, both the structural S2 subunit, as well as both of the two functional S1 subunits. [328] This binding of all 3 subunits of the trimeric spike protein may be considered a trifecta of fortunate results of ivermectin in favor of the human host and in opposition to the SARS-CoV-2 virus.
Ivermectin has different mechanisms against parasites, already a miraculous healing drug for that use alone through much of the world’s population. However, now that we learn of its tremendous effect in binding both RdRp and all three trimers of the spike protein of SARS-CoV-2, we are certainly fortunate to have this medicine in our arsenal against COVID-19. It is inexpensive, and full COVID-19 treatment of an individual, from first dose till last needed can be less than one US dollar. Ivermectin is therefore available to even the poorest communities in the world. Ivermectin is being compared to the discovery of penicillin in its enormous impact, and perhaps was one of the greatest discoveries of the 20th century. [329] The fact that this tremendously effective, safe and low-cost antiviral drug is not as thoroughly known to the world as penicillin is a chasm of inexcusable and deadly ignorance that the COVID era is giving the world an opportunity to correct.
Reposted from the author’s Substack
References
309 K Sharun, K Dhama, et al. Ivermectin, a new candidate therapeutic against SARS-CoV-2/COVID-19. May 30 2020. Ann Clin Microbiol Antimicrob. 19 (23). https://annclinmicrob.biomedcentral.com/articles/10.1186/s12941-020-00368-w
310 Covid Analysis. Ivermectin is effective for COVID-19: Real-time meta-analysis of 49 studies. Nov 26 2020. Updated Mar 31 2021. https://ivmmeta.com/
311 J Rajter, M Sherman, et al. Use of ivermectin is associated with lower mortality in hospitalized patients with coronavirus disease 2019: The ivermectin in COVID nineteen study. Jan 2021. Chest. 159 (1). 85-92. https://www.sciencedirect.com/science/article/pii/S0012369220348984
312 R Chahla, L Ruiz, et al. Ivermectin repurposing for COVID-19 treatment of outpatients in mild stage in primary health care centers. Mar 30 2021. MedRxiv. https://www.medrxiv.org/content/10.1101/2021.03.29.21254554v1
313 H Tanioka, S Tanioka, et al. Why COVID-19 is not so spread in Africa: How does Ivermectin affect it? Mar 26 2021. MedRXiv. https://www.medrxiv.org/content/10.1101/2021.03.26.21254377v1.full-text
314 T Jabeen, M Khader, et al. A review on the anti-parasitic drug ivermectin for various viral infections and possibilities of using it for novel severe acute respiratory syndrome coronavirus 2: New hope to treat coronavirus disease – 2019. Jun 2020. Asian J Pharm Clin Res. https://www.researchgate.net/publication/343742900_A_REVIEW_ON_THE _ANTIPARASITIC_DRUG_IVERMECTIN_FOR_VARIOUS_VIRAL_INFECTIONS_AND_POSSIBILITIES_OF_USING_IT_FOR_NOVEL_SEVERE_ACUTE_RESPIRATORY_SYNDROME_CORONAVIRUS_2_NEW_HOPE_TO_TREAT_CORONAVIRUS_DI SEASE
315 J Sanz-Navarro, C Feal, et al. Treatment of human scabies with oral ivermectin. Sep 2017. Actas Dermos. 108 (7). 643-649. https://pubmed.ncbi.nlm.nih.gov/28385424/
316 J Remme, R Baker, et al. A community trial of ivermectin in the onchocerciasis focus of Asubende, Ghana. I: Effect on the microfilarial reservoir and the transmission of Onchocerca volvulus. Sep 1989. Trop Med Parasitol. 40 (3). 367-374. https://pubmed.ncbi.nlm.nih.gov/2617046/
317 M Pacqué, B Muñoz, et al. Pregnancy outcome after inadvertent ivermectin treatment during community-based distribution. Dec 15 1990. Lancet. 336 (8729). 1486-1489. https://pubmed.ncbi.nlm.nih.gov/1979100/
318 US FDA. FAQ: COVID-19 and ivermectin intended for animals. Dec 16 2020. https://www.fda.gov/animal-veterinary/product-safetyinformation/faq-covid-19-and-ivermectin-intended-animals
319 R Croci, E Bottaro, et al. Liposomal systems as nanocarriers for the antiviral agent ivermectin. May 8 2016. Int J Biomater. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4875998/
320 M Yagisawa, P Foster, et al. Global trends in clinical studies of ivermectin in COVID-19. Mar 10 2021. Japanese J Antibiotics. 74 (1). 44-95. http://jjacontents.wdc-jp.com/pdf/JJA74/74-1-open/74-1_44-95.pdf
321 L Caly, J Druce, et al. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Jun 2020. Antiviral Res. https://www.sciencedirect.com/science/article/pii/S0166354220302011?via%3Dihub
322 M Turkia. A timeline of ivermectin-related events in the COVID-19 pandemic. Mar 2021. https://www.researchgate.net/publication/350496335_A_Timeline_of_Iver mectin-Related_Events_in_the_COVID-19_Pandemic
323 I Udofia, K Gbayo, et al. In silico studies of selected multi-drug targeting against 3CLpro and nsp12 RNA-dependent RNA-polymerase proteins of SARS-CoV-2 and SARS-CoV. Mar 25 2021. Network Mod Anal Health Inf Bioinf. 10 (22). https://link.springer.com/article/10.1007/s13721-02100299-2
324 L Caly, J Druce, et al. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Jun 2020. Antiviral Res. https://www.sciencedirect.com/science/article/pii/S0166354220302011?via%3Dihub
325 M Tay, J Fraser, et al. Nuclear localization of dengue (DENV) 1-4 nonstructural protein 5; protection against all 4 DENV serotypes by the inhibitor ivermectin. Sep 2013. Antivir Res. 99 (3). 301-306. https://www.sciencedirect.com/science/article/abs/pii/S0166354213001599
326 K Wagstaff, H Sivakumaran, et al. Ivermectin is a specific inhibitor of importin alpha/beta-mediated nuclear import able to inhibit replication of HIV-1 and dengue virus. May 1 2012. J Biochem. 443 (3). 851-856. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3327999/
327 S Yang, S Atkinson, et al. The broad spectrum antiviral ivermectin targets the host nuclear transport importin alpha/beta1 heterodimer. May 2020. Antivir Res. 104760. https://www.sciencedirect.com/science/article/abs/pii/S0166354219307211
328 A Choudhury, N Das, et al. Exploring the binding efficacy of ivermectin against the key proteins of SARS-CoV-2 pathogenesis: an in silico approach. Future Vir. Mar 25 2021. https://www.futuremedicine.com/doi/10.2217/fvl-2020-0342
329 M Yagisawa, P Foster, et al. Global trends in clinical studies of ivermectin in COVID-19. Mar 10 2021. Japanese J Antibiotics. 74 (1). 44-95. http://jjacontents.wdc-jp.com/pdf/JJA74/74-1-open/74-1_44-95.pdf
The Truth About Ivermectin
Medical miracle or notorious lynchpin of misinformation?
Nov 21 2022
Ivermectin has been hailed as a “wonder drug” and, according to the UNESCO World Science Report, a critical component of “one of the most triumphant public health campaigns ever waged in the developing world.”
However, since the onset of the COVID-19 pandemic, the National Institutes of Health (NIH) and affiliated health authorities have vociferously recommended against ivermectin as a potential treatment for the virus.
Though the Food and Drug Administration (FDA) has approved ivermectin for human use in treating conditions caused by parasites, it has also insisted that ivermectin “has not been shown to be safe or effective” when it comes to treating COVID-19.
In a social media message that has gone viral, the FDA labeled it as a drug for horses and not fit for human consumption: “You are not a horse. You are not a cow. Seriously, y’all. Stop it.”
The post made headlines and was one of the FDA’s most successful social media campaigns. Yet, research findings seem to contradict the public health organization’s recommendations.
A growing body of research shows that ivermectin is an essential treatment for COVID-19. Many doctors have praised the drug for its broad yet effective antiparasitic, antiviral, antibacterial, anti-inflammatory, anti-cancer, and autophagic properties.
Ivermectin: Antiparasitic Beginnings
Ivermectin made its name through its significant benefits in treating parasitic infections.
In 1973, Satoshi Omura and William C. Campbell, working with the Kitasato Institute in Tokyo, found an unusual type of Streptomyces bacteria in Japanese soil near a golf course.
In laboratory studies, Omura and Campbell discovered that this Streptomyces bacteria could cure mice infected with the roundworm Heligmosomoides polygyrus. Campbell isolated the bacteria’s active compounds, naming them avermectins, and the bacteria was thus called S. avermitilis.
Despite decades of searching worldwide, researchers have yet to find another microorganism that can produce avermectin.
It was changing one of the bonds of avermectin through a chemical process that produced ivermectin, which was proven successful in treating onchocerciasis and lymphatic filariasis, both of which are debilitating diseases common in the developing world.
A portrait of William Campbell and an illustration describing his work displayed on a screen during a press conference of the 2015 Nobel Medicine Prize. William Campbell and Satoshi Omura won the Nobel Medicine Prize for their discoveries of treatments against parasites—Avermectin, which was modified to Ivermectin. (JONATHAN NACKSTRAND/AFP via Getty Images)
Though its broad antiparasitic functions are not well understood, it is known that ivermectin penetrates parasites’ nervous systems, turning off their neurons’ actions, possibly deactivating and killing them.
As part of a donation campaign launched in 1988 by Merck & Co., Inc., the manufacturer of ivermectin, the drug was used in Africa to treat river blindness. Also called onchocerciasis, river blindness is a tropical disease caused by Onchocerca volvulus worms. It is the second-most common cause worldwide of infectious blindness.
The Onchocerca worms mature in the skin of an infected individual (“the host”). After mating, female worms can release into the host’s skin up to 1,000 microfilariae a day; the female worms live for 10 to 14 years. The presence of these worms can lead to scarring in the tissues and, when microfilariae invade the eye, can cause visual impairment or complete loss of vision.
The World Health Organization estimates that 18 million people are infected globally, and 270,000 have been blinded by onchocerciasis.
When Merck distributed ivermectin in areas hardest hit by the disease, treatment benefited the residents’ overall health and led to economic recovery. Ivermectin replaced previous drugs that had devastating side effects.
“Ivermectin proved to be virtually purpose-built to combat Onchocerciasis,” Omura wrote in a study he co-authored in 2011.
Ivermectin has also proven effective against lymphatic filariasis, known as elephantiasis. Parasitic worms transmitted through the bite of an infected mosquito can grow and develop in lymphatic vessels, which regulate the body’s water balance. When certain vessels are blocked, the areas—typically the legs and genitals—can swell, with the legs enlarging to elephant-like stumps.
Worldwide, more than 120 million people are infected, 40 million of whom are seriously incapacitated and disfigured.
The World Health Organization listed ivermectin as an essential drug and has advised many countries to run annual campaigns to rid people of these parasites. Such recommendations are a solid testament to ivermectin’s safety.
For their work, including the discovery of avermectin, in 2015, Omura and Campbell were among three recipients of the Nobel Prize in Physiology or Medicine.
It is an indispensable drug for the underdeveloped world, with about 3.7 billion doses administered as part of global campaigns during the past 30 years. To this day, ivermectin remains a staple drug of tropical areas and an essential drug in treating onchocerciasis, lymphatic filariasis, strongyloidiasis, and scabies.
Ivermectin and COVID-19
Analyses of studies on ivermectin have found it effective as a prevention, a treatment for acute COVID-19, and in advanced stages of infection by the virus.
- Ivermectin as a Prophylaxis
Prophylaxis intervenes in the first phases of COVID-19 infection, which is mainly asymptomatic, when the virus replicates to increase its viral load—symptom onset occurs after the viral load peaks.
Ivermectin can be effective in the early stages of infection. Outside the cells, ivermectin can attach to parts of the virus, immobilizing it and preventing it from entering and infecting human cells.
Ivermectin can also enter the cell to prevent the virus from replicating. SARS-CoV-2 needs cell replication machinery to make more of the virus; ivermectin attaches and blocks a protein critical to this process, preventing viral production.
Additionally, ivermectin can be absorbed from the skin and stored in fat cells for a long time.
“Because it’s lipid soluble, it is stored and slowly released, [so] once you’ve taken a prophylactic dose, and I think it’s like the cumulative dose of about 400mg, that your risk of getting COVID is close to zero and you can actually stop it for a while,” said Dr. Paul Marik, a widely published critical care specialist with 500 peer-reviewed papers to his name, in an interview with The Epoch Times. Marik co-founded the Front Line COVID-19 Critical Care Alliance (FLCCC), a group of physicians formed in the early days of the pandemic and dedicated to treating COVID-19. According to interviews, many of the group’s doctors have successfully treated COVID-19 with ivermectin. The organization’s other co-founder, Dr. Pierre Kory, has written a book about ivermectin’s use and controversy during the pandemic.
Dr. Sabine Hazan, a gastroenterologist with 22 years of experience in clinical research, told The Epoch Times that she would advise ivermectin use for only a short time in critical patients rather than recommending the use of it as a prophylaxis. Continuous use of ivermectin—as with all drugs—can make the body dependent on the drug rather than working to fix itself.
- Ivermectin for Early and Acute COVID
Many peer-reviewed studies have found that ivermectin, when used by itself or in conjunction with other therapies in symptomatic patients, reduces ventilation time, time for recovery, and the risk of progressing to severe disease. (pdf 1, pdf 2, pdf 3)
This is likely due to ivermectin’s anti-inflammatory role in multiple pathways, achieved by clearing out the viral particles by immobilizing them, reducing inflammation, and improving mitochondrial action.
Suppose the early viral replication is not controlled and cleared out soon enough by the body’s immune system. In that case, the infection can become severe or even hyperinflammatory, possibly leading to systemic organ failures.
Ivermectin can also directly interact with immune pathways, suppressing inflammation and reducing the chances of developing a cytokine storm. A cytokine storm occurs when the immune system is hyperactive and hyperinflammatory. Though ivermectin can help to clear out the virus and its particles, the inflammatory state of the tissues and the organs can often cause more damage than the virus itself.
Ivermectin also likely improves gut health, which plays an essential role in immunity by preventing bacteria and viruses from infecting people via the gut.
In a published study, Hazan hypothesized that ivermectin helps COVID-19 patients by increasing the levels of Bifidobacteria—a beneficial bacteria—in the gut.
As the CEO and founder of her own genetic sequencing research laboratory, ProgenaBiome, Hazan noticed that the Bifidobacteria levels in her stools would increase after she took ivermectin. Critical COVID patients would have “zero Bifidobacteria,” which can often be a sign of poor health.
In her peer-reviewed study on hypoxic patients, she observed that COVID patients with low oxygen levels from the cytokine storms in their lungs would improve within hours of administering ivermectin.
“When people die of COVID, they die from the cytokines—they couldn’t breathe anymore. It’s almost like an anaphylactic reaction. So when you give them ivermectin at the moment they’re about to crash, you’re boosting the Bifidobacteria [and increasing their oxygen],” Hazan said.
She explained that ivermectin is a fermented product of Streptomyces bacteria. Streptomyces are within the same group Bifidobacteria are from, which may explain why ivermectin temporarily boosts Bifidobacteria.
Ivermectin also helps with mitochondrial function. During severe COVID-19, patients often experience pulmonary dysfunctions due to lung inflammation, reducing oxygen flow. This can cause stress to the mitochondria, leading to fatigue, and, when severe, may cause cell and tissue death. Ivermectin has been shown to increase energy production, indicating that it is beneficial to the mitochondria.
Furthermore, Ivermectin can bind to the spike protein—a distinctive structural feature of the COVID virus which has a crucial role in its pathogenesis. In systemic disease, the spike protein can enter the bloodstream and bind to red blood cells to form blood clots. Ivermectin can prevent blood clots from forming in the body.
- Ivermectin for Long COVID and Post-Vaccine Symptoms
The number of studies supporting ivermectin to treat long COVID and post-COVID-19 vaccine symptoms is limited. However, doctors treating these conditions have observed successful results with ivermectin.
An Argentinian study published in March 2021 is the only peer-reviewed study evaluating ivermectin for long COVID.
Researchers found that in patients reporting long COVID symptoms—including coughing, brain fog, headaches, and fatigue—ivermectin alleviated their symptoms.
Mechanistically, ivermectin can improve autophagy. This process is usually switched off during COVID-19 infections. By switching autophagy back on, ivermectin can help cells clear remnant viral proteins out, returning stability to the cell.
Like acute and severe COVID-19, chronic spike protein triggers inflammation, and ivermectin can reduce such responses by suppressing inflammatory pathways and lessening the damage to tissues and blood vessels.
The Changing Public Health Messaging on Ivermectin
The NIH’s stance on ivermectin has changed several times.
Early in the pandemic, there was little information on ivermectin as a potential treatment for the virus.
The first study that mentioned ivermectin as a potential COVID-19 treatment came from Australia in April 2020. Researchers administered ivermectin to SARS-CoV-2-infected monkey kidney cells in the laboratory and found the drug beneficial. However, the researchers concluded that further study was needed. Many health agencies, including the NIH, the CDC, and other global health regulators concluded that ivermectin could kill the virus only at toxic levels.
Even now, NIH’s statement on ivermectin for COVID-19 reads: “Ivermectin has been shown to inhibit replication of SARS-CoV-2 in cell cultures. However, pharmacokinetic and pharmacodynamic studies suggest that achieving the plasma concentrations necessary for the antiviral efficacy detected in vitro would require administration of doses up to 100-fold higher than those approved for use in humans.”
In October 2020, the first clinical study showing the benefits of ivermectin was published by the journal CHEST. The study found ivermectin to reduce mortality rates in COVID-19 patients and garnered immediate attention.
The study’s lead author, Dr. Jean-Jacques Rajter, is a critical care doctor specializing in pulmonary medicine.
Rajter gave a testimony (pdf) of his findings to the Senate Committee on Homeland Security & Governmental Affairs in December 2020.
The day after he saw the Australian study, one of his COVID patients dramatically deteriorated from breathing normally at room oxygen levels to requiring intubation. The patient’s son pleaded with Rajter to save his mother using whatever options were available. Dr. Rajter recognized that hydroxychloroquine would be ineffective in the advanced stages of COVID. After much deliberation, Dr. Rajter tried ivermectin.
“The patient deteriorated as expected for about 12 more hours but stabilized by 24 hours and improved by 48 hours. After this, two more patients had similar issues and were treated with the ivermectin-based protocol. Based on experience, these patients should have done poorly, yet they all survived,” the testimony read.
More clinical studies were published, showing the benefits of ivermectin as a prophylactic treatment. (pdf 1, pdf 2).
The findings encouraged the use of ivermectin among doctors desperate to find a cure.
Meanwhile, by October 2020, research into COVID-19 vaccines and the use of remdesivir to treat the virus was already in full swing.
According to the FDA, specific criteria should be met for the EUA (Emergency Use Authorization) to be granted for vaccines and medications, including that there are “no adequate, approved, and available alternatives.”
Some doctors say that if ivermectin’s use for COVID had been approved, it would have made the EUAs for vaccines and remdesivir null and void.
Following the Australian study, the FDA published a statement, “FAQ: COVID-19 and Ivermectin Intended for Animals,” highlighting the use of ivermectin in animals and advising against the use of ivermectin for COVID-19.
The NIH also discouraged the use of ivermectin, albeit briefly. On Jan. 14, 2021, the NIH changed its statement, writing that there was no evidence to recommend or disapprove the use of ivermectin. However, in April 2022, the statement changed to strongly disapproving of using ivermectin.
“We [Marik, Kory, and Dr. Andrew Hill, a virologist and consultant to the WHO] had a conference with NIH in January of 2021. We presented our data, and Andrew Hill presented the data he had done…there were a number of studies at that point, which were very positive,” said Marik.
Health Authority Overreach
Despite the NIH’s neutral statement on ivermectin for most of 2021, the FDA actively campaigned against using ivermectin in COVID-19 patients. On Aug. 26, 2021, the CDC sent an emergency warning against using ivermectin; a few weeks later, the American Medical Association and affiliated associations called for an end to ivermectin use.
Many doctors were thus discouraged from using ivermectin, and pharmacies refused to prescribe it. State health agencies warned against using ivermectin, and medical boards removed the medical licenses of doctors who prescribed ivermectin, alleging misinformation.
Yet using the FDA’s statement against ivermectin to ban its use in COVID-19 cases would be considered an overreach. Since the FDA approved ivermectin in 1996, this made the drug acceptable for off-label use.
“The fact that it’s not FDA approved for COVID is irrelevant because the FDA endorses the use of off-label drugs at the clinician’s discretion,” said Marik.
As an ironic side effect of the messaging on ivermectin, people suddenly found themselves unable to access ivermectin, and some turned to veterinary-grade ivermectin.
Though veterinary ivermectin is the same product as medicinal ivermectin, the manufacturing standard is not the same as it is for human-grade pharmaceuticals.
Contradictory Research and Campaigns
Though the initial research in 2020 showed promising results for ivermectin, published studies reported conflicting findings by the following year.
The NIH has funded many studies on the effectiveness of ivermectin, the most recent being ACTIV-6.
Individuals can participate in the study once they develop COVID by selecting ivermectin from four other drugs. The drug was sent to them via mail. This method means that some people in the study could have recovered by the time they received the ivermectin.
There are some controversies regarding this study.
The first is that the authors changed the primary endpoints during the study, which is heavily frowned upon as it can affect the validity and reliability of the outcome.
Initially, the primary endpoint was the number of deaths, hospitalizations, and symptoms reported at day 14.
This was changed to the number of deaths, hospitalizations, and symptoms by day 28. In the actual published study, there was another change, with the endpoint being duration of COVID-19 symptoms.
A rapid review published by the Massachusetts Institute of Technology (MIT) implied that the endpoints were changed because, by the time the study commenced, there were far fewer events of death and hospitalizations; as a result, there would not be enough data for a reliable comparison.
Indeed, the data at the ACTIV-6 livestream showed that the ivermectin group reported only one death; this death would not be considered relevant to the research because the patient was hospitalized and died before he took ivermectin.
There were also further implementations in the study that could impact the observed effectiveness of the drug.
On average, this study’s participants received treatment six days after first reporting symptoms. Patients needed to report eligible symptoms and test positive for COVID-19 before receiving drugs. Due to this added time, about seven percent of the participants had no symptoms by the time ivermectin arrived.
Despite these negative findings for ivermectin, there is still some evidence that may demonstrate that ivermectin can be useful in treating COVID-19.
In the abstract, the authors concluded that taking ivermectin had “a posterior probability of benefit of .91,” this is another way of writing that ivermectin had a 91 percent probability of being more beneficial than placebo.
The percent of probability is below 95 percent, making the benefit of ivermectin insignificant.
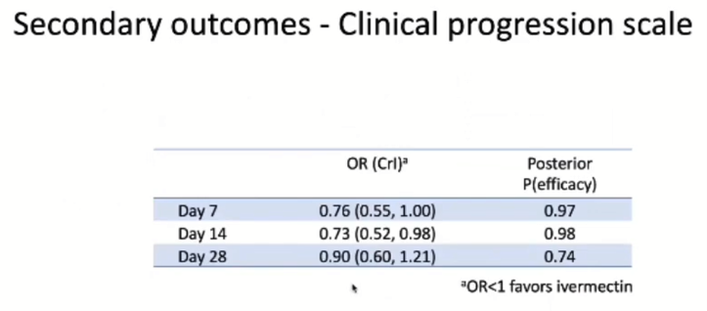
Slides from the ACTIV-6 presentation on a statistically significant secondary endpoint findings.
Another secondary endpoint showed that by day 14, ivermectin already had a statistically significant 27 percent benefit with 98 percent probability of efficacy.
The FDA and NIH did not respond for comments by press time.
The War on Ivermectin
The outcome could have been much different - and many lives saved - if Big Pharma hadn't been so successful at suppressing this generic pharmaceutical that was found to work against COVID-19.
Story-at-a-Glance
- In his book, “The War on Ivermectin: The Medicine That Saved Millions and Could Have Ended the COVID Pandemic,” Dr. Pierre Kory details the history of ivermectin and the how and why behind Big Pharma’s suppression of this drug when it was found to work against COVID-19
- After spending his career as an internist and critical care physician, Kory has now turned his attention to long-haul COVID and post-jab injury syndromes
- Daily ivermectin use is a mainstay of the treatment plans for long-haulers and those with COVID jab injuries, as the drug very effectively binds to the toxic spike protein that is causing most of the damage in both of these conditions
- Methylene blue can be helpful for those struggling with crippling fatigue, as it boosts mitochondrial respiration and improves energy metabolism. It’s actually the parent molecule for hydroxychloroquine and chloroquine, off-patent drugs used to treat COVID-19 along with zinc
- “The War on Ivermectin” reveals the disinformation playbook used by Big Pharma and its many allies to suppress highly useful and inexpensive medicines in order to protect and increase corporate profits
In this interview, return guest Dr. Pierre Kory discusses his new book, “The War on Ivermectin: The Medicine That Saved Millions and Could Have Ended the COVID Pandemic.” In it, he details the history of ivermectin and the how and why behind Big Pharma’s suppression of this drug when it was found to work against COVID-19.
Like Dr. Paul Marik and Dr. Peter McCullough, Kory has been threatened by the American Board of Internal Medicine, which is seeking to yank his medical license. While a family doctor in private practice can operate without board certification, most medical centers will not hire a doctor who isn’t board certified in his specialty, and insurance companies won’t put you on their panel.
Kory’s Response to the American Board of Internal Medicine
Kory, however, is not overly concerned about this threat — which is really little more than an intimidation tactic to shut him up — as he has no intention of ever going back to a hospital setting.
“I’m done,” he says. “There’s no way I could walk into a hospital. I’ve just learned too much. I’ve learned too much about pharmaceutical control of almost all of the medical evidence. There’s no way I can fit. Now I’m a square peg in a round hole.
So, to be honest, I don’t think [losing my board certification] would have an impact. I am now in private practice. I have a bustling telehealth practice and I’m very happy. I’m outside the system, I can do and say and care for the patients in a manner that I best see fit.
Anyway, our reply [to the American Board of Internal Medicine] was different than Peter’s. He presented all the evidence to support all the statements they accused him of as being misinformation; very data driven, evidence-based.
What we did is, our lawyer looked at their policy on misinformation and the process of ‘convicting’ someone of misinformation, and it required that they provide us the evidence showing that we are wrong and misinformed.
But the letter to us was bizarre. It was this hodgepodge of statements that I’d made or written on my Substack, and it was just implied that that’s misinformation …
So, we wrote back very simply, ‘Excuse us, but your letter does not follow your own misinformation policy. We ask that you kindly reissue the letter with the evidence showing that we’re wrong.’ And we’ve gotten radio silence ever since.”
Kory’s New Specialty
After spending his career as an internist and critical care physician, Kory has now turned his attention to long-haul COVID and post-jab injury syndromes — complex chronic illnesses. To that end, he’s collaborating with doctors who’ve spent decades treating other tricky conditions, such as chronic Lyme disease, fibromyalgia and chronic fatigue syndrome.
“So, not only do I have a new career and practice, but also a new intellectual focus and it’s much more satisfying. I’m literally returning people to levels of function that they weren’t at before.
These were oftentimes healthy people with full careers, children, they exercised, ate right and now they’re fully disabled with numerous organ system complaints.
And I’ll tell you, getting them from 20% [function] to 40% [function] is a big deal, when they can actually do just a little bit more than they were doing before, and when you get them to 80%, it’s transformative.
But it’s way more challenging. And I tell my patients, ‘Listen, I have to be humble here. I’m trying to figure this out. I’m collaborating, I’m reading, I’m learning from you.’ I’m learning from each patient, because we’re doing a lot of empiric therapies.
We’re trying things, and so I learn. Each patient serves as their own control and I’m finding different things work on different patients. But the real challenge that I’m finding is that I don’t have any biomarkers or tests that I find helpful to direct therapies.
A lot of the tests are normal, even inflammatory markers. Clotting markers are normal, and yet I know that they have inflammatory processes and they’re thrombogenic. So, I wish there was more research and guidance.”
Treating Long-Haul COVID
One of the primary complaints of those struggling with what we’re now calling “long-haul COVID” is fatigue, a lack of energy to do even the most basic things. Since mitochondria are responsible for 90% of the energy production in your body, it stands to reason that impaired energy production in the mitochondria, or more simply, mitochondrial dysfunction, is at play.
The challenge is how to recover that function. One fascinating drug that can help in this regard is methylene blue, which helps mitochondrial respiration and improves brain energy metabolism. Methylene blue is actually the parent molecule for hydroxychloroquine and chloroquine, off-patent drugs commonly used to treat not only malaria but also COVID-19.
Best known as a fish tank antiseptic and textile dye for blue jeans, it was actually the first synthetic drug in modern history, developed in 1876. Since then, we’ve discovered it has many really important medicinal benefits. Importantly, it’s the only known antidote for metabolic poisons, i.e., any poison that interferes with oxygen transport or displaces oxygen, either from the blood or from the mitochondria.
Christian-Driven America-First Precious Metals.
Before markets collapse, the smart play is to move wealth or retirement to precious metals. Contact Genesis Gold now to make it happen smoothly with no hassles from a group driven by fellowship.
Basically, as an electron cycler, methylene blue acts like a battery, but unlike other compounds that do the same thing, it doesn’t cause damaging oxidation in the process. You can review my interview with Dr. Francisco Gonzalez Lima here for more information.
If anything interferes with oxygenation or cellular respiration, such as cyanide, methylene blue is able to bypass that point of interference through electron cycling, thus allowing mitochondrial respiration, oxygen consumption and energy production to function as it normally would. And, the effect is typically felt within hours, as it increases, by about 30%, the ability of the mitochondria to produce ATP in the electron transport chain. Kory has also found it useful.
“My really sick patients use methylene blue,” he says. “Some of the really sick ones that aren’t responding to medicine, I send to a clinic where they do apheresis, ozone, methylene blue, infrared. One of them actually was discharged on oral methylene blue. And so, I want to figure out how to implement oral methylene blue.”
Trial and Error
Methylene blue is far from a cure-all, however. Any number of processes could be impacting your mitochondria, and they all need to be addressed. Adding to the complexity is that remedies that work really well in one long-hauler or COVID jab-injured patient often will not work for another, even though they present with very similar symptoms.
“We’ve [found] about six or seven different pathophysiologic mechanisms, and one of them is mitochondrial dysfunction, but I don’t know which is the predominant one in each patient,” Kory says. “I have no way of figuring that out. The only way I figure it out is by responses to therapy.
For instance, I had one young woman recently. I tried a number of therapies and what resurrected her, finally, was when I started to treat mast cell activation. I put her on antihistamine, famotidine [a heartburn medication], ketotifen [an asthma medication], and Boom.”
The Case for Sun Exposure
Daily sun exposure for about an hour around solar noon can also be important, as the near-infrared wavelengths will trigger melatonin production in your mitochondria, where you need it the most.
Melatonin is a potent antioxidant, so getting plenty of sunshine on bare skin is a simple way to reduce reactive oxygen species (ROS) that cause damage, and secondarily increase the efficiency of ATP production. Kory has been recommending this as well.
COVID Really Revealed the Level of Corruption in Science
During our conversation, the issue of medical journals came up, and their role in the corruption of science. Kory notes:
“That’s the other transformation that Paul [Marik] and I have undergone. We really looked to those journals thinking they were the most sophisticated and that was the top levels of science. But seeing what was published in those journals throughout COVID uncovered the absolute control by the pharmaceutical industry.
I mean, what appears in those journals is what they allow to appear in those journals. Period. I know of many positive studies of repurposed drugs rejected. We’ve seen them pull the following — JAMA and The New England Journal both — where instead of rejecting [the paper] they hold onto it as if they’re considering it, and then the rejection comes months later.
I’ve never heard of that in my career. Usually, when I’ve tried to submit manuscripts, they either say, ‘This is interesting. We’re sending it out for peer review,’ or they say, ‘This is not of sufficient interest to our readership at this time.’
They rejected positive trials of ivermectin. And then, probably the greatest and most saddening corruption that they pulled, is that they published the Together trial on ivermectin, which is so brazenly fraudulent and corrupt.
There are so many documented actions those investigators took in order to ensure they did not have a statistically significant benefit for ivermectin. Yet the New England Journal of Medicine published it. When you look at the design and the conduct of the trial, it should never be published. It was brazenly corrupt.
The investigators were all working for either their own companies or other companies whose sole job was to do research contracts for pharmaceutical companies. I mean, what would happen in their careers had they published a positive trial on ivermectin? That’s it. Bye. No more contracts.”
The War on Ivermectin
According to Kory, the idea for “The War on Ivermectin” was birthed after reading an article titled “The Disinformation Playbook,”1 published by the Union for Concerned Scientists. He explains:
“What happened is that after my ivermectin testimony2 [December 8, 2020, before Sen. Ron Johnson], which went viral and brought a lot of attention to the FLCCC … our protocols were looked in to. Doctors started prescribing ivermectin.
And I thought — this is how naive I was — I literally thought that we were providing a major intervention that would alter the trajectory of the pandemic, without question. It would reduce cases, hospitalizations and deaths, and now you have an effective early outpatient treatment. And I thought that news would be welcomed.
I thought the FLCCC would come out as heroes. It was really Paul who identified the data signal first. He said, ‘Wow. You got to see what these studies are starting to show.’ I jumped in right behind him. I was the first author of that comprehensive review paper.
I worked a lot and I got deeply expert on ivermectin. But what happened in the next few months is that everything started going sideways, and I could not figure it out. I saw hit pieces. To you, this is not news. You’re probably like, ‘Yep. I’ve seen that before.’
The thing is, I didn’t know. I didn’t know that what I was really doing — bringing forth data supporting the efficacy of a generic drug — that is poking the bear. And when I say poking the bear, what is anathema to the pharmaceutical industry and their whole business model is they cannot have generic off-patent drugs become standard of care. It obliterates the market for their pricing new pills.
I didn’t know I was stepping into a war. In the history of pharma, I don’t think any single medicine threatened as many [drug] markets and campaigns. The only other medicine that did that was hydroxychloroquine, but they already killed hydroxychloroquine in 2020.
I was coming out now with ivermectin, and it threatened hundreds of billions of dollars in perpetuity for these insanely lethal vaccines, monoclonal antibodies, remdesivir, paxlovid, molnupiravir — all of the markets for their novel new pills to enter. I mean, I don’t think any medicine has ever threatened that much of a market.
So, we were getting attacked. I did an interview with the Associated Press and the article that came out, I mean, I almost had a heart attack [reading it]. I saw unending attacks on ivermectin and it was coming in different directions. I saw academia getting all hot and bothered.
‘It’s a fringe medicine. It’s unproven. The trials are small.’ I saw all these narratives and I didn’t know they were narratives at the time. I thought people were being stupid … Now, I see everything. I see everything they do now, even before they do it, because they’re really predictable.”
The Disinformation Playbook
The turning point came when Kory received a two-line email from Dr. William B. Grant (who also co-wrote my review paper3 on vitamin D for COVID prevention). The email said, “Dr. Kory, what they’re doing to ivermectin is what they’ve done to vitamin D for decades.” Attached was a link to The Disinformation Playbook article.4
“It’s a short article. It’s very well-designed. They have little diagrams and then they have examples of disinformation campaigns. They describe the five plays, which they name after American football plays. And these are the tactics that pharma used. I read the article and I was like, ‘Yes. Yes. Yes. Yes. Yes.’
Suddenly, the world made sense — and not in a good way. It was very ugly, because I was like, ‘That’s what’s going on. There’s a massive disinformation campaign directed at ivermectin.’ From that moment on, everything that happened, every day, it was almost like I got tied to a front row seat for a horror movie. I’ve had to watch a horror movie unfold ever since.
Millions dying, hospitals overflowing. And there’s a drug that could prevent that. It could avert catastrophe. It would’ve definitely either put the brakes on or stopped the vaccine campaign obsession, which is in my mind, is one of history’s greatest humanitarian catastrophes.
It’s a holocaust out there with these vaccines. That’s easily proven from immense sources of data now, from life insurance data, disability data, excess mortality data. Now we’re even seeing birth rates dropping.
So, the theme of the book is centered around that. It’s my experiences and knowledge of what they do … It’s almost like a teacher’s manual, because I saw everything they pulled, how they did it and how successful they were — the fire plays, the blitz, harass the scientists that come out with inconvenient science, the diversion, inject doubt where there is none.”
Indeed, these disinformation tactics have a long history. They’re not new. It’s just that people in general have not been aware of these tactics, so they worked like a charm and could be used over and over again.
Disinformation Is an Old PR Tool Used by Toxic Industries
In the 1950s, the tobacco industry hired a PR agency called Hills and Knowlton, which established all the strategies Kory just listed and discuss at depth in his book. The tobacco industry used it so effectively, they were able to quash cancer concerns for another 50 years.
Their disinformation campaign didn’t end until attorneys general across the country finally decided to collaborate and bring massive lawsuits against the tobacco industry, winning not only settlements but also — and more importantly — limiting their ability to practice disinformation through media and advertising.
The telecommunications industry has used the same tactics since the ’90s. They actually hired the same PR firm to protect their business and hoodwink customers, and they’re still going strong. Unlike tobacco, which was finally understood to cause cancer, electromagnetic field (EMF) exposure from cell phones and Wi-Fi is still not recognized as a biological danger, despite massive amounts of evidence.
The drug industry, though, has perhaps used the disinformation playbook the longest, and it’s high time to break their magic spell. The way we do that is by educating ourselves and others about how they use disinformation to manipulate you. Once you know their playbook, it’s like being equipped with X-ray vision.
“I think ‘The War on Ivermectin’ is almost as important as Bobby Kennedy’s book, ‘The Real Anthony Fauci,’ where he, in a highly-referenced fashion, documents the control of medicine and the medical sciences and how it’s literally controlled by pharma and how depraved that control is,” Kory says.
“They do not care. The pharmaceutical industry is a documented criminal industry. They’ve released many, many products that have caused untold deaths and what do they do? They try to suppress that evidence for as long as possible. They get caught. They pay a fine. They do it again.”
Academic Freedom Is an Illusion
Kory also became wise to the fact that these kinds of medical disinformation campaigns have been routine for decades. Ivermectin was just the last in a long line of repurposed drugs that were being suppressed, lest it threaten Big Pharma profits. Cancer drugs, heart medications and psychiatric remedies have all been buried in the same way. He continues:
“So, I started to learn about how pharma practices disinformation, and I think the most terrible disinformation campaigns, which caused more deaths than any other, were the ones on hydroxychloroquine and ivermectin …
So, the book is about all of the tactics that I witnessed. It’s also about my personal journey. I’ve been through a lot. I’ve lost three jobs. One I left voluntarily. One was mutual. The third was a firing. Also, my proudest contribution to COVID [was writing what] I thought was the best paper of my life. It was a paper that argued that the pulmonary phase of COVID is actually an organizing pneumonia, or what they used to call BOOP.
I wrote a paper with one of the top chest radiologists in the world. I consulted pathologists. I looked at autopsy data, even just the CAT scans were in a pattern of organized pneumonia, which is a terrible descriptor for the disease, because it suggests that it’s an infection and it’s not.
Organizing pneumonia is an inflammatory response to a lung injury. The gold standard of care is corticosteroids. That’s the only thing that’s been shown to really reverse organized pneumonia.
I gave testimony in the Senate in May 2020, telling the world that it was critical to use corticosteroids in the hospital phase of disease. I got attacked by the University of Wisconsin. By the way, you know another thing that I learned? Academic freedom isn’t real. As soon as you’re a professor with an opinion that goes against orthodoxy or the system, oh, you’re going to feel the pressure …
I was vindicated on corticosteroids. It’s now the standard of care around the world. However, the standard of care dose is 6 milligrams of dexamethasone, which is too low, [and] methylprednisone is far superior in its effects on the lung.
It’s well-known that in fulminant cases, like whited out lungs on a ventilator, you need … 1,000 milligrams of methylprednisone for three days in a row. Six milligrams of Dex is equivalent to about 32 milligrams of methylprednisone.”
COVID Hospitalizations Eradicated With Ivermectin
While there are many individual success stories out there, one that Kory believes best illustrates the power of ivermectin against COVID is that of Itajai, Brazil, a city of 220,000 people. In June 2020, they implemented a prophylaxis program using ivermectin. The program was advertised throughout local media, and people were encouraged to participate and take ivermectin four times a month, on days 1, 2, 15 and 16.
On the appropriate days, they set up tents and centers where people could get the drug, and the entire program was carefully logged in an electronic database. In all, 159,000 Brazilians participated, of those 113,000 elected to take the ivermectin. Kory and eight coauthors published a paper5 on the results in March 2022.
“The 113,000 [who took the ivermectin] were older, sicker, fatter. Way more cardiovascular disease and diabetes. And, obviously, they were probably more worried about the impacts on their health.
So, when you look at that comparison, I mean, there are massive negative confounders. But despite those confounders, even when you didn’t propensity match, there were insanely positive benefits in the ivermectin group.
They died much less, I think it was 70% lower risk of dying, 68% lower risk of hospitalization and 50% lower risk of getting COVID. And that was in the sickest of the sick in that city. Then, when we did propensity matching, matching them for age and other things, it was even greater.
There’s a follow up study which is astounding, where … they were able through pharmacy records to split the ivermectin group into two. Regular ivermectin users, those who took all their pills, and irregular, those who missed doses.
And when you look at the regular users, the ones who were most adherent to the protocol, no one went to the hospital. There was a 100% reduction in hospitalization and a 90% lower risk of dying. It’s astounding … I’ve never seen a more proven therapy in any disease model, which they successfully got everyone to believe is a horse dewormer used by unvaccinated conspiracy theorists.”
Dosage Recommendations
Ivermectin recommendations have changed over time, as newer variants have acted differently, requiring updated approaches. At present, Kory still recommends ivermectin for prevention, if you really feel you need it. Current COVID variants are very mild, however, and rarely cause severe problems (unless you got the COVID jab).
For those struggling with long-haul COVID, ivermectin is a mainstay. “It’s the most frequently effective therapy,” Kory says. “I do have in my practice a minority who are ivermectin non-responders, but the majority respond in either small or large ways.” Importantly, ivermectin is the most effective drug available for binding to the spike protein.
So, if there’s circulating spike protein in your body, be it from natural infection or the jab, ivermectin will help bind to it, thereby preventing much of the spike’s negative impacts.
Ivermectin also repolarizes macrophages from the M1 to the M2 subtype. M1 is hyperinflammatory and M2 is hypo-inflammatory. So, it reduces inflammation. In addition to that, ivermectin has at least 18 other mechanisms of action and downstream effects that can be helpful.
Covid variant BA.5 is spreading. It appears milder but much more contagious and evades natural immunity. Best to boost your immune system with new Z-Dtox and Z-Stack nutraceuticals from our dear friend, the late Dr. Vladimir Zelenko.
For long-haulers and the COVID jab injured, Kory typically starts patients out at 0.3 mg per kilo of bodyweight once a day. For most, that dose works well. It’s still unclear how long people need to stay on this daily dose. Oftentimes, when they try to cut back, symptoms return, which suggests they still have spike protein in their bodies. Fortunately, the safety profile of ivermectin, even for long-term use, is very good.
Save the Date: Medical Conference in Orlando, October 2022
Hopefully, more doctors will get involved in the treatment of spike protein injuries. October 15 and 16, 2022, the Front Line COVID-19 Critical Care Alliance (FLCCC) will be holding a medical conference in Orlando, Florida, titled “Understanding and Treating Spike Protein Induced Diseases.” You can register for the conference on the FLCCC’s website.
“We have a lineup of speakers, deeply studied in treatment of complex chronic illnesses from different specialties. There are a lot of ways to approach this disease, so it’s really important. It really is directed at the treating providers. Because one of the many abject failures is they literally don’t recognize vaccine injury.
There’s no clinic for the vaccine injured. They’re abandoned, and I’m just going to be crude here — they’re pissing off the doctors because all of these patients are showing up that doctors have no idea what’s wrong with.
They have no knowledge of the mechanisms. They have no knowledge of what some effective therapies can be. So, they’re not treating these patients. They’re abandoned and gaslit.
Some doctors actually get angry when the patients relate their symptoms to the vaccine. They don’t want to hear it. They don’t want a vaccine injured in their practice. I have numbers of patients where the physician literally told them, ‘You don’t need to schedule a follow up.’
So, for those [doctors] who still have a shred of humanity, empathy and understanding that the spike protein is a toxin that causes immense amounts of disease, I hope they attend and/or watch the lectures that we’ll stream afterwards.
We’re coming at this very humble. I mean, there are very few trials on therapies in these two syndromes. So, it’s really about clinical knowledge, expertise and experiences from this disease and other diseases.
I am looking forward to it because I want to learn. I want to listen to those other speakers and hear about what they think and how they approach this. And I think it’s going to be a really tremendous conference. I think a lot of laypeople will show up too …
Laypeople who are much more deeply studied and knowledgeable on what’s really going on. They didn’t go to medical school, but they’re deeply studied and they read papers. They watch, read a lot of data sources.
So, I think it would be of interest to laypeople who want to learn how to either help themselves, or help their friends and colleagues, just like they did with COVID. You know how many laypeople passed around our protocols and tried to get their friends and relatives access to the medicines on our protocol? They saved lives. They saved lives by doing that.”
More Information
In the interview, Kory also reviews the clear and present danger the COVID jab poses to women, especially if they’re pregnant or want to get pregnant in the future. We also review the blatant fraud perpetrated by Pfizer to hide the massive number of miscarriages that occurred in its human trial.
In summary, the miscarriage rate is 87.5%, which is just astounding. No woman in her right mind would pull that trigger if she had that information. We also discuss the worldwide drops in birth rates (which began after the rollout of these experimental jabs), the complete absence of any supporting data for the authorization of COVID shots for children (which is yet another medical fraud perpetrated on the American people), and the lie that COVID is a pandemic of the unvaccinated (it’s actually the complete opposite).
So, for more on those topics, please listen to the full interview, or read through the transcript. You can also find more of Kory’s work on PierreKory.substack.com. Last but not least, be sure to pick up a copy of “The War on Ivermectin: The Medicine That Saved Millions and Could Have Ended the COVID Pandemic” to learn all about how the biggest, most lethal medical disinformation play was perpetrated, right before your eyes.
Article cross-posted from Dr. Mercola’s Substack.
New ivermectin study shows 92% lower chance of COVID death
Protection increases with increased usage of politically charged drug
By Art Moore
Published August 31, 2022 at 7:24pm
A large study on the impact of using ivermectin as a prophylaxis for COVID-19 found that regular users of the drug experienced up to a 92% reduction in mortality compared to those who did not.
Brazilian research scientist Dr. Flavio A. Cadegiani said via Twitter that his study in his home country showed a "dose-response effect," meaning that "the more you used, the more protection you had."
He observed that people who use ivermectin regularly every 15 days for at least six to eight weeks had up to a 92% reduction in mortality.
Cadegiani conducted a previous study of drug that evaluated whether its use could impact COVID-19 infection and mortality rates.
Last fall, esteemed epidemiologist Dr. Harvey Risch of Yale Medical School was among scientists and physicians who said in Senate testimony that thousands of lives could have been saved if treatments such as ivermectin and hydroxychloroquine had not been suppressed.
For 25 years, WND has boldly brought you the news that really matters. If you appreciate our Christian journalists and their uniquely truthful reporting and analysis, please help us by becoming a WND Insider!
In April, after noticing that the word ivermectin was trending on Twitter amid Elon Musk's move to buy the company, the FDA reprised its disingenuous "horse dewormer" smear of the drug as a treatment for COVID-19.
"Hold your horses, y'all. Ivermectin may be trending, but it still isn't authorized or approved to treat COVID-19," said a post on the FDA's Twitter account.
The reference to horses played on the explosion last fall of media articles and social media posts mocking people who treated COVID-19 with the drug as ignorant rubes who were sneaking into farms or patronizing Tractor Supply stores in quest of "horse dewormer."
During the pandemic, Twitter and other social media platforms censored positive mention of ivermectin and hydroxychloroquine despite the countless testimonies and dozens of studies from around the world showing the drugs to be effective in treating COVID-19.
A follow-up FDA post said: "Also, a reminder that a study showed it didn't actually work against COVID."
Dr. Pierre Kory, who has testified to the Senate of the effectiveness of ivermectin against COVID-19, fired back.
"You are not a horse, you are not a cow, you are Big Pharma's ass," he tweeted.
The FDA, he wrote, was "messaging BS" by citing "one corrupt study" while ignoring 82 trials, including 33 randomized controlled trials with 129,000 patients from 27 countries that show "massive benefits" of ivermectin in treating COVID-19.
"Stop lying man, people are dying," he wrote, adding the hashtag "earlytreatmentworks."
In an article published in April for the Brownstone Institute, Kory wrote that it's "a tried-and-true tactic with effective and dastardly results" for "Big Pharma and other well-financed interests" to sponsor purportedly impartial medical trials "aimed at discrediting cheaper generic alternatives.'
"Ignoring the flaws in the methodology, the media runs wild with the desired narrative, which is amplified by a well-orchestrated public relations effort," he wrote.
Kory cited as an example the newly reported clinical trial from Brazil known as "TOGETHER," which he said ostensibly aimed at studying the effectiveness of ivermectin to treat COVID.
Among the flaws was the lack of explicit exclusion criteria for trial participants on ivermectin, meaning both trial groups had access to the same drug. Further, the treatment window was set for only three days, which didn't allow for adequate dosing, and the trial was conducted during the massive gamma variant surge, which was one of the most virulent and deadly COVID variants.
"The dosage of the trial was far lower than everyday Brazilian clinicians were prescribing patients at the time to match the strength of the strain," Kory pointed out.
"In spite of these and other readily apparent shortcomings, the nation’s leading media gobbled up the results. 'Ivermectin Didn't Reduce Covid-19 Hospitalizations in Largest Trial to Date' blared the Wall Street Journal, while a New York Times headlined announced, 'Ivermectin Does Not Reduce Risk of Covid Hospitalization, Large Study Finds.'"
Meanwhile, social media platforms stifled conversations while California pushed potentially precedent-setting legislation to punish doctors "who dare question phony studies," threatening loss of a medical license.
A similar study of ivermectin "of far larger size, conducted by investigators without any conflicts of interest, found the drug led to massive reductions in Covid infection, hospitalization and mortality—yet it received virtually no media coverage."
Kory said that ending "this cycle of perpetual disinformation requires revamping our dysfunctional drug approval process."
"An independent board free of pharma industry conflicts must be established to oversee trials for re-purposed medicines," he said. "Recommendations should be based on trials designed by impartial experts and actual results, not the desired ones, and policymakers or prescribers who ignore the findings should be held accountable."
And academia and the regulatory agencies must be reminded, he said, "that observational trials data – wherein a sample of population who take a drug are compared to those who do not – is equally valid at informing policy."
"Randomized controlled trials can yield useful information, but their complexity, costs, and delays to treatment lead to errors and effectively shut out low-cost drugs from the approval process, regardless of their efficacy," he said.
Shocking Conclusions from Africa Study Expose Why Big Pharma’s Puppets are Suppressing Ivermectin Data
The vaccine-nannies are busy saying Ivermectin doesn't work, but they don't look to the science to show this. They simply gaslight us about the "horse dewormer."
by JD Rucker
Joe Rogan, Kirstie Alley, and a handful of other celebrities have brought out the anti-Ivermectin wolves in America. Mainstream media is in full attack-mode. Big Tech is censoring posts to the point that people are coming up with creative ways to indicate they’re even talking about Ivermectin so as not to trigger the filters. The CDC claimed the drug was for horses only, neglecting to remove their own recommendations for people to take Ivermectin for other issues.
If the CDC is recommending what they deemed to be a “horse dewormer” to people traveling from Africa, does that mean the CDC is racist?
A graph made its rounds on social media yesterday that raised some eyebrows. It showed the clear difference between countries in Africa that use Ivermectin regularly versus those that do not. The differences were startling as the Ivermectin-nations showed unambiguous advantages against Covid-19. The mortality rates were very low compared to countries that do not use Ivermectin on a wide scale.
This graph prompted me to dig deeper into the study. As it turned out, the graph is the tip of the iceberg. There are other data points supporting the use of Ivermectin as a treatment for Covid-19 scattered throughout the study. I’ll publish the whole thing below, but here are some important takeaways for easy digestion.
First, the countries that use Ivermectin have less-sophisticated medical facilities than the nations that do not use Ivermectin. This means that life expectancy is lower and testing is more sporadic. Universal Ivermectin use seems to be the only factor preventing these nations from a full-blown Covid-19 catastrophe.
Second, Africa seems to be the perfect environment for this type of study because of the stark differences in mortality rates. Nations that push Ivermectin as an antiparasitic agent were not attempting to fight Covid-19. They’ve been using the drug universally for years. Therefore, the data regarding mortality clearly delineates between Ivermectin nations and non-Ivermectin nations. As the study states, “The community-directed onchocerciasis treatment with ivermectin is the most reasonable explanation for the decrease in morbidity and fatality rate in Africa.”
The final and arguably most important “hidden” takeaway from the study is that recovery and fatality rates for Covid-19 cases were not statistically significantly different between Ivermectin countries and non-Ivermectin countries. That means that once a person was tested and officially declared a Covid-19 case, they recovered or died at essentially the same rates across the board.
This tells us that other factors such as medical proficiency, environmental differences, or access to vaccines do not contribute to whether someone lives or dies once they have become sick with the disease. Since overall mortality rates per capita are significantly lower in Ivermectin nations but case fatality rates are the same, Ivermectin is clearly effective as an early treatment and perhaps even as a preventative measure.
Remember, the people in the Ivermectin nations are already taking the drug. They aren’t waiting for a positive Covid test and likely aren’t even very concerned about the disease at all. Many if not most who do end up becoming Covid-19 cases in Ivermectin nations were likely among those who were not taking Ivermectin as an antiparasitic. This is why they’re on equal footing when they go to the hospital as those living in non-Ivermectin nations.
Here is the study. Below it, I will offer some commentary on what this all means for America and the rest of the world.
Why COVID-19 is not so spread in Africa: How does Ivermectin affect it?
Hisaya Tanioka, Sayaka Tanioka, Kimitaka Kaga
Abstract
Background Scientists have so far been unable to determine the reason for the low number of COVID-19 cases in Africa.
Objective To evaluate the impact of ivermectin interventions for onchocerciasis on the morbidity, mortality, recovery, and fatality rates caused by COVID-19.
Method A retrospective statistical analysis study of the impact of ivermectin against COVID-19 between the 31 onchocerciasis-endemic countries using the community-directed treatment with ivermectin (CDTI) and the non-endemic 22 countries in Africa. The morbidity, mortality, recovery rate, and fatality rate caused by COVID-19 were calculated from the WHO situation report in Africa. We investigated the onchocerciasis endemic 31 countries and the non-endemic 22 countries. Statistical comparisons used by the Welch test of them in the two groups were made.
Results The morbidity and mortality were statistically significantly less in the 31 countries using CDTI. The recovery and fatality rates were not statistically significant difference. The average life expectancy was statistically significantly higher in the non-endemic countries.
Conclusions The morbidity and mortality in the onchocerciasis endemic countries are lesser than those in the non-endemic ones. The community-directed onchocerciasis treatment with ivermectin is the most reasonable explanation for the decrease in morbidity and fatality rate in Africa. In areas where ivermectin is distributed to and used by the entire population, it leads to a significant reduction in mortality.
Introduction
At least for now, it seems that Africa will be in completely different situations under the coronavirus infections. Some scientists have cited a higher proportion of young people [1,2], a warmer climate [3], and widespread BCG vaccination [4] as possible factors. While these are positive theories, they do not provide scientific evidence to explain why the spread of new coronavirus infections in Africa appears to be at a slower pace than in other parts of the world.
In the meantime, based on a growing data of recently reported data on a large number of published and unpublished trials, it is suggested that ivermectin being a well-known antiparasitic agent with antiviral activity and anti-inflammatory effects, has activity against SARS-CoV-2 [5]. On the other hand, ivermectin has been administered in Africa for onchocerciasis under the WHO strategy. In 2012, WHO’s neglected tropical diseases (NTD) Roadmap set a goal of elimination where feasible by 2020, and the African Programme for Onchocerciasis Control advanced the goal to elimination in 80% of countries by 2025 [6].
The community-directed treatment with ivermectin (CDTI) is the basic strategy to eradicate onchocerciasis in Africa. More than 99% of the infections have occurred in the 31 countries in Sub-Saharan Africa listed below: Angola, Benin, Burkina Faso, Burundi, Cameroon, Central Africa, Chad, Republic of Congo, Cote d’Ivoire, Democratic Republic of Congo, Equatorial Guinea, Ethiopia, Gabon, Ghana, Guinea, Guinea-Bissau, Kenya, Liberia, Malawi, Mali, Mozambique, Niger Nigeria, Rwanda, Senegal, Sierra Leone, South Sudan, Sudan, Togo, Uganda, Tanzania. In the rural populations of sub-Saharan Africa where health systems are weak and under-resourced, the community-directed treatment strategy is proving to be one of Africa’s most successful in reducing disease at low cost [7].
If ivermectin has an antiviral effect on SARS-CoV-2, the morbidity, mortality, recovery, and fatality rates caused by COVID-19 would be reduced in the community-directed treatment with ivermectin (CDTI) countries compared to non-endemic untreated ones. Therefore, epidemiological analyzes of the two groups are necessary. These results will validate the effect of ivermectin intervention on COVID-19. This study aims to evaluate the impact of ivermectin interventions for onchocerciasis on morbidity, mortality, recovery rate, and fatality rate caused by COVID-19.
Materials
We divided into two group countries. One was 31 onchocerciasis-endemic countries (Ivermectin group) using the community-directed treatment with ivermectin (CDTI), and the other was 22 non-endemic countries (non-Ivermectin group). Each population and average life expectancy were obtained from the WHO Africa statics in 2019 [8]. The COVID-19 data was obtained from the WHO coronavirus disease Dashboard on January 15, 2021, and the COVID-19 Situation update for the WHO African Region [9]. Each morbidity, mortality, recovery rate, and fatality rate caused by COVID-19 were calculated from the collected data.
Table 1 showed the population (in millions), morbidity (number of cases and per million population), mortality (number of deaths and per million population), recovery rate (number of cases and percentage), and fatality rate (percentage) in the onchocerciasis-endemic 31 countries. Table 2 showed them in the non-endemic 22 countries.
Analytical method
This study aimed to verify the ivermectin intervention statistics in the community-directed treatment with ivermectin. Therefore, we compare the morbidity, mortality, recovery rate, and fatality rate caused by COVID-19 between the two group countries.
Statistical Analysis
Statistical analysis was done by Microsoft Excel 2016 (Microsoft Corporation Redmond, Washington). Data were presented as a mean and standard deviation (SD) and compared between the two groups utilizing Welch-test. A two-sided P value < 0.05 was considered significant.
Results
The results of the onchocerciasis-endemic of 31 countries (Ivermectin group) and the non-endemic 22 countries (non-Ivermectin group) were shown in Table 3.
Morbidity and mortality were statistically significantly less in the ivermectin group. The population, recovery rate, and fatality rate were not statistically significant differences between them. The average life expectancy was statistically significantly high in the non-ivermectin group.
Discussion
It is important to verify the effect of ivermectin interventions on the variations in morbidity and mortality and the associated viral lethality. Ivermectin is an approved antiparasitic drug that is used to treat several neglected tropical diseases, including onchocerciasis, helminthiases, and scabies. For these indications, ivermectin has been widely used and has demonstrated an excellent safety profile [10].
This epidemiological study in Africa reveals that the morbidity and mortality in the onchocerciasis-endemic countries (Ivermectin group) are statistically lesser than those in the non-endemic ones (non-Ivermectin group). However, the morbidity will depend on the number of COVID-19 tests. Onchocerciasis-endemic countries are mainly in the medically weak areas in Sub-Saharan Africa rather than the non-endemic countries. Therefore, the average life is statistically different between the two groups. And, we suggest that the number of COVID-19 tests in the endemic-countries will be lesser than the non-endemic ones because their health systems are under-resourced.
In other words, the apparent incidence of COVID-19 may be lower in the onchocerciasis-endemic countries, but mortality is unrelated to the number of tests. The mortality is less in the ivermectin group than the non-ivermectin one. The recovery and fatality rates are statistically the same in both groups, although they will depend on the medical circumstances. That is, is the medical situation not that different between the two group countries, or is there another factor at play?
Some researchers say that the short life expectancy and the fact that 3% of the population is over 65 years old may be a reason for COVID-19 not exploding infections in Africa [1, 2]. The mean age of the average life expectancy in epidemic countries is 60.7 years and 66.4 years in non-epidemic countries. However, countries with shorter average life expectancy have worse medical circumstances than countries with longer average life expectancy. As a result, the epidemic countries have higher infant mortality and lower average life expectancy [8]. And more, if this difference is one of the factors in the impact, the statistically no difference in the recovery rate and fatality rate between the two groups shows a discrepancy.
Taking this into account, mortality is lower in ivermectin-treated countries than those in non-treated ones. The recovery rate and fatality rate may be improved according to the number of COVID-19 tests. These results imply that ivermectin will act on SARS-CoV-2, and prevent deterioration in patients. Our results will support those of Mohammad et al.’s study [11].
On the other hand, the South African Health Products Regulatory Authority (SAHPRA) has given the green light for the controlled use of Ivermectin for humans on January 27, 2021 [12]. Since then, the number of new COVID-19 infections in South Africa has been declining.
In conclusion, in the countries where ivermectin is distributed to and used by the entire areas, it suggests to lead a reduction in mortality, to accelerate patient recovery and, to avoid death. And this analytical study will suggest that early treatment with ivermectin may accelerate recovery and prevent worsening of symptoms in patients with mild disease. These findings can be efficiently translated into therapies for SARS-CoV-2 (COVID-19).
Ethical approval
Ethical approval was not required for this work as public data analysis.
Funding
No funding was received.
Competing interests
The authors have no competing or conflicting interests.
Authors’ contributions
H.T., S.T., and K.K. conceived and designed the study. H.T. and S.T. analyzed the data and wrote the first draft. All authors provided critical revisions. All authors contributed equally to this study and approved the submitted manuscript.
References
- Age, Sex, Existing Conditions of COVID-19 Cases and Deaths-Worldometer. Available at https://www.worldometers.info/coronavirus/coronavirus-age-sex-demographics/ Accessed February. 18, 21.
- Mehta NS, Mytton OT, Mullins EWS, et al. SARS-CoV-2 (COVID-19): What Do We Know About Children? A Systematic Review. Clin Infect Dis. 2020 Dec 3;71(9):2469–2479. doi: 10.1093/cid/ciaa556.
- Iqbal MM, Abid I, Hussain S, et al. The effects of regional climatic condition on the spread of COVID-19 at global scale. Sci Total Environ. 2020 Oct 15; 739: 140101. doi: 10.1016/j.scitotenv.2020.140101.
- Malik YS, Ansari MI, Ganesh B, et al. BCG vaccine: a hope to control COVID-19 pandemic amid crisis. Hum Vaccin Immunother. 2020 Dec 1;16(12):2954–2962. doi: 10.1080/21645515.2020.1818522. Epub 2020 Sep 29.
- IVERMECTIN —A Potential global solution to the COVID-19 pandemic. FLCCC Alliance · October 31, 2020. Available at ivermectin_1.pdf (kitasato-infection-control.info) Accessed February 27, 2021.
- WHO | Regional Office for Africa. Onchocerciasis. Available at https://www.afro.who.int/health-topics/onchocerciasis
- WHO | African Programme for Onchocerciasis Control (APOC). Available at https://www.who.int/apoc/cdti/en/
- United Nations: Population and Vital Statistics Report. Population, latest available census, and estimates, latest available data. (Last Updated: 15 January 2021) Available at https://unstats.un.org/unsd/demographic-social/products/vitstats/seratab2.pdf
- Weekly epidemiological update – 19 January 2021. WHO African Region. Available at https://www.who.int/publications/m/item/weekly-epidemiological-update 19-january-2021
- Canga AG, Prieto AMS, Liébana MJD, et al. The Pharmacokinetics and Interactions of Ivermectin in Humans—A Mini-review. AAPS 10 (1); 42–46 (2008) DOI: 10.1208/s12248-007-9000-9CrossRefPubMedWeb of Science
- Ahmed S, Karim MM, Ross AG, et al. A five-day course of ivermectin for the treatment of COVID-19 may reduce the duration of illness. Int J Infect Dis. 2021 Feb; 103: 214–216. doi: 10.1016/j.ijid.2020.11.191. Epub 2020 Dec 2.
- South Africa Government News Agency. SAHPRA approves Ivermectin for controlled human use. Available at https://www.sanews.gov.za/south-africa/sahpra-approves-ivermectin-controlled-human-use
Commentary
When Anderson Cooper et al take to the airwaves to say Ivermectin is a horse dewormer, they are being disingenuous, though there’s actually a silver lining to their lies. There is a difference between the Ivermectin one can get at a feed store and the Ivermectin prescribed to humans. Though their intention in gaslighting us on the drug was to ridicule those who recommend it, at least they gave us an opportunity to tell people to find a doctor to prescribe it and NOT to go to the local farm supply store to take livestock versions of the drug.
Nevertheless, mainstream media is lying. Big Tech “fact checkers” are lying. The CDC is lying. Those who are taking to social media to “debunk” the efficacy of Ivermectin are either lying or ignorant. This is the point in the story where I’m supposed to ask why so many are denying the clear science supporting Ivermectin in favor of gaslighting, but I won’t ask. You already know the answer.
The push for universal vaccinations is the only priority right now for just about everyone in government, media, Big Tech, academia, and even the leftist trolls on social media. Ivermectin has always been the Achilles Heel for vaccine-pushers which is why they are willing to denigrate their own credibility to keep information about it suppressed. The MATH+ Protocols have shown tremendous success in treating Covid-19, but you’ll never hear Anthony Fauci mention them.
The powers-that-be can gaslight us with tortured numbers and media proclaiming Ivermectin is just a “horse dewormer,” but they cannot get around the Africa study. It’s the silver bullet, proof-positive that Ivermectin works.
Dr. Terry Rickard
The FDA's War Against The Truth On Ivermectin
WEDNESDAY, OCT 20, 2021 - 07:30 PM
Authored by David Henderson and Charles Hopper via The American Institute for Economic Research,
On July 28, the Wall Street Journal ran our article “Why Is the FDA Attacking a Safe, Effective Drug?”
In it, we outlined the potential value of the antiparasitic drug ivermectin for Covid-19, and we questioned the FDA’s vigorous attack on ivermectin. Many people praised us and many criticized us. We had clearly covered a sensitive subject. It didn’t help that one of the studies we referenced was retracted the day our article was published. Within hours of learning that fact, we sent a mea culpa to the Journal’s editors. They acted quickly, adding a note at the end of the electronic version and publishing our letter. It’s important to address two criticisms of our work. The first is that we exaggerated the FDA’s warning on ivermectin. The second is that Merck’s stance on ivermectin proved that even the company that developed ivermectin thought that it doesn’t work for Covid-19.
First, we didn’t exaggerate the FDA’s warning on ivermectin.
Instead, the agency changed its website after our article was published, probably to reflect the points we made.
Second, Merck had two incentives to downplay ivermectin’s usefulness against the novel coronavirus.
We’ll explain both points more fully.
Ivermectin was developed and marketed by Merck & Co. while one of us (Hooper) worked there years ago. Dr. William C. Campbell and Professor Satoshi Omura were awarded the 2015 Nobel Prize for Physiology or Medicine. They earned it for discovering and developing avermectin. Later Campbell and some associates modified avermectin to create ivermectin. Merck & Co. has donated four billion doses of ivermectin to prevent river blindness and other diseases in areas of the world, such as Africa, where parasites are common. The ten doctors who are in the Front Line Covid-19 Critical Care Alliance call ivermectin “one of the safest, low-cost, and widely available drugs in the history of medicine.” Ivermectin is on the WHO’s List of Essential Medicines and ivermectin has been used safely in pregnant women, children, and infants.
Ivermectin is an antiparasitic, but it has shown, in cell cultures in laboratories, the ability to destroy 21 viruses, including SARS-CoV-2, the cause of Covid-19. Further, ivermectin has demonstrated its potential in clinical trials for the treatment of Covid-19 and in large-scale population studies for the prevention of Covid-19.
Contradicting these positive results, the FDA issued a special statement warning that “you should not use ivermectin to treat or prevent Covid-19.” The FDA’s warning, which included language such as, “serious harm,” “hospitalized,” “dangerous,” “very dangerous,” “seizures,” “coma and even death,” and “highly toxic,” might suggest that the FDA was warning against pills laced with poison. In fact, the FDA had already approved the drug years ago as a safe and effective anti-parasitic. Why would it suddenly become dangerous if used to treat Covid-19? Further, the FDA claimed, with no scientific basis, that ivermectin is not an antiviral, notwithstanding its proven antiviral activity.
Interestingly, at the bottom of the FDA’s strong warning against ivermectin was this statement: “Meanwhile, effective ways to limit the spread of COVID-19 continue to be to wear your mask, stay at least 6 feet from others who don’t live with you, wash hands frequently, and avoid crowds.” Was this based on the kinds of double-blind studies that the FDA requires for drug approvals? No.
After some critics claimed that we overstated or overreacted to the FDA’s special warning, we reviewed the FDA’s website and found that it had been changed, and there was no mention of the changes nor any reason given. Overall, the warnings were watered down and clarified. We noticed the following changes:
- The false statement that “Ivermectin is not an anti-viral (a drug for treating viruses)” was removed.
- “Taking a drug for an unapproved use can be very dangerous. This is true of ivermectin, too” was changed to the less alarming “Ivermectin has not been shown to be safe or effective for these indications.” (Indications is the official term used in the industry to denote new uses for a drug, such as new diseases or conditions, and/or new patient populations.)
- The statement, “If you have a prescription for ivermectin for an FDA-approved use, get it from a legitimate source and take it exactly as prescribed,” was changed to, “If your health care provider writes you an ivermectin prescription, fill it through a legitimate source such as a pharmacy, and take it exactly as prescribed.” This more clearly acknowledges that reasonable physicians may prescribe ivermectin for non-FDA-approved uses, such as Covid-19.
- The ending statement about masks, spacing, hand washing, and avoiding crowds was replaced with one that recommended getting vaccinated and following CDC guidelines.
- The reasonable statement “Talk to your health care provider about available COVID-19 vaccines and treatment options. Your provider can help determine the best option for you, based on your health history” was added at the end.
The new warning from the FDA is more correct and less alarming than the previous one.
In a statement from February, Merck, the company that originated and still sells ivermectin, agreed with the FDA that ivermectin should not be used for Covid-19.
“We do not believe that the data available support the safety and efficacy of ivermectin beyond the doses and populations indicated in the regulatory agency-approved prescribing information.”
To some, this appeared to be a smoking gun. Merck wants to make money, they reason, and people are interested in using ivermectin for Covid-19, therefore, Merck would warn against such usage only if the scientific evidence were overwhelming. But that’s not how the pharmaceutical industry works.
Here’s how the FDA-regulated pharmaceutical industry really works.
The FDA judges all drugs as guilty until proven, to the FDA’s satisfaction, both safe and efficacious. By what process does this happen? The FDA waits for a deep-pocketed sponsor to present a comprehensive package that justifies the approval of a new drug or a new use of an existing drug. For a drug like ivermectin, long since generic, a sponsor may never show up. The reason is not that the drug is ineffective; rather, the reason is that any expenditures used to secure approval for that new use will help other generic manufacturers that haven’t invested a dime. Due to generic drug substitution rules at pharmacies, Merck could spend millions of dollars to get a Covid-19 indication for ivermectin and then effectively get zero return. What company would ever make that investment?
With no sponsor, there is no new FDA-approved indication and, therefore, no official recognition of ivermectin’s value. Was the FDA’s warning against ivermectin based on science? No. It was based on process. Like a typical bureaucrat, the FDA won’t recommend the use of ivermectin because, while it might help patients, such a recommendation would violate its processes. The FDA needs boxes checked off in the right order. If a sponsor never shows up and the boxes aren’t checked off, the FDA’s standard approach is to tell Americans to stay away from the drug because it might be dangerous or ineffective. Sometimes the FDA is too enthusiastic and these warnings are, frankly, alarming. Guilty until proven innocent.
There are two reasons that Merck would warn against ivermectin usage, essentially throwing its own drug under the bus.
Once they are marketed, doctors can prescribe drugs for uses not specifically approved by the FDA. Such usage is called off-label. Using ivermectin for Covid-19 is considered off-label because that use is not specifically listed on ivermectin’s FDA-approved label.
While off-label prescribing is widespread and completely legal, it is illegal for a pharmaceutical company to promote that use. Doctors can use drugs for off-label uses and drug companies can supply them with product. But heaven forbid that companies encourage, support, or promote off-label prescribing. The fines for doing so are outrageous. During a particularly vigorous two-year period, the Justice Department collected over $6 billion from drug companies for off-label promotion cases. Merck’s lawyers haven’t forgotten that lesson.
Another reason for Merck to discount ivermectin’s efficacy is a result of marketing strategy. Ivermectin is an old, cheap, off-patent drug. Merck will never make much money from ivermectin sales.
Drug companies aren’t looking to spruce up last year’s winners; they want new winners with long patent lives.
Not coincidentally, Merck recently released the clinical results for its new Covid-19 fighter, molnupiravir, which has shown a 50% reduction in the risk of hospitalization and death among high-risk, unvaccinated adults. Analysts are predicting multi-billion-dollar sales for molnupiravir.
While we can all be happy that Merck has developed a new therapeutic that can keep us safe from the ravages of Covid-19, we should realize that the FDA’s rules give companies an incentive to focus on newer drugs while ignoring older ones. Ivermectin may or may not be a miracle drug for Covid-19. The FDA doesn’t want us to learn the truth.
The FDA spreads lies and alarms Americans while preventing drug companies from providing us with scientific explorations of existing, promising, generic drugs.
Dr. Terry Rickard

Search our Site...



